Вам также может понравиться
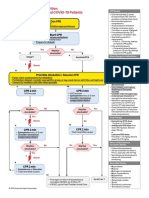
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsДокумент1 страницаACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoОценок пока нет
- Covid 19 CPR 7 RulesДокумент21 страницаCovid 19 CPR 7 RulesMiguel Cuevas DolotОценок пока нет
- Effectiveness of Transdermal MagnesiumДокумент2 страницыEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Covid 19 CPR 7 RulesДокумент21 страницаCovid 19 CPR 7 RulesMiguel Cuevas DolotОценок пока нет
- How Can Patients Visitors Help - May18Документ2 страницыHow Can Patients Visitors Help - May18Miguel Cuevas DolotОценок пока нет
- PSB 368Документ6 страницPSB 368Miguel Cuevas DolotОценок пока нет
- Covid 19 PDFДокумент18 страницCovid 19 PDFMiguel Cuevas DolotОценок пока нет
- Physical Examination in ENT: Ussana Promyothin, MDДокумент60 страницPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotОценок пока нет
- (MED) COVID-19 Trans V. 2.0Документ6 страниц(MED) COVID-19 Trans V. 2.0Isabel VinasОценок пока нет
- Physical Examination in ENT: Ussana Promyothin, MDДокумент60 страницPhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotОценок пока нет
- Vertigo Gail Ishiyama 1 13 10Документ40 страницVertigo Gail Ishiyama 1 13 10Myname Rama LienОценок пока нет
- Anesthesia Pocket Cards 7 18 18Документ6 страницAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotОценок пока нет
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Документ30 страницClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmОценок пока нет
- Physical Assessment: Ear, Nose, Mouth, and ThroatДокумент59 страницPhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotОценок пока нет
- Clinical AbstractДокумент4 страницыClinical AbstractMiguel Cuevas DolotОценок пока нет
- Cook Book (Filipino) 13 PDFДокумент23 страницыCook Book (Filipino) 13 PDFAdina AnghelОценок пока нет
- Pedia Tickler Update 2017Документ2 страницыPedia Tickler Update 2017Tani BokОценок пока нет
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFДокумент12 страницA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotОценок пока нет
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFДокумент12 страницA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotОценок пока нет
- Active Listening HANDOUT PDFДокумент26 страницActive Listening HANDOUT PDFMiguel Cuevas DolotОценок пока нет
- Drug IndexДокумент2 страницыDrug IndexMiguel Cuevas DolotОценок пока нет
- Neurologic ExamДокумент1 страницаNeurologic ExamMiguel Cuevas DolotОценок пока нет
- HEMAreviewДокумент3 страницыHEMAreviewMiguel Cuevas DolotОценок пока нет
- Benign Paroxysmal Positional Vertigo: Waseem WatadДокумент37 страницBenign Paroxysmal Positional Vertigo: Waseem WatadnoviОценок пока нет
- Nocturnals Physiology 2018Документ14 страницNocturnals Physiology 2018Miguel Cuevas DolotОценок пока нет
- History Taking ExaminationДокумент7 страницHistory Taking ExaminationIndunil AnuruddhikaОценок пока нет
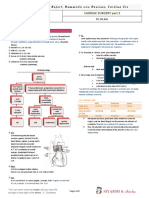
- TCVS - Cardiac Surgery Part 2 Dr. de AsisДокумент8 страницTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotОценок пока нет
- Kerosene PDFДокумент31 страницаKerosene PDFRudyMLanaОценок пока нет
- Community-Acquired Pneumonia - CPG 2016Документ26 страницCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- ICU One Pager Chest TubesДокумент1 страницаICU One Pager Chest TubesMohamed MahmoudОценок пока нет
- PBL Respi 1 Week 1Документ6 страницPBL Respi 1 Week 1FrinkaWijayaОценок пока нет
- Ventilators, Intensive CareДокумент48 страницVentilators, Intensive CarealetripoleОценок пока нет
- Test Bank Chapter 26: Nursing Assessment: Respiratory SystemДокумент11 страницTest Bank Chapter 26: Nursing Assessment: Respiratory SystemMonicaОценок пока нет
- Artificial RespirationДокумент26 страницArtificial RespirationAbdul RehmanОценок пока нет
- CopdДокумент29 страницCopdRidha SyahputraОценок пока нет
- Curriculum Respiratory Medicine 2020 21Документ47 страницCurriculum Respiratory Medicine 2020 21Naresh KumarОценок пока нет
- Asthma and COPD NCLEXДокумент17 страницAsthma and COPD NCLEXPotchiee PfizerОценок пока нет
- Active Cycle Breathing TechniqueДокумент20 страницActive Cycle Breathing TechniqueRAM100% (2)
- The Basics of Respiratory Mechanics: Ventilator-Derived ParametersДокумент11 страницThe Basics of Respiratory Mechanics: Ventilator-Derived ParametersAntonioLonigroОценок пока нет
- Attachment PDFДокумент2 страницыAttachment PDFYuyus Dwi PrasetiyoОценок пока нет
- Case StudyДокумент7 страницCase StudyKarl Benedic GarciaОценок пока нет
- Tube ThoracostomyДокумент13 страницTube ThoracostomyzahraaОценок пока нет
- Bikker Ido Geert BEWERKTДокумент167 страницBikker Ido Geert BEWERKTDara Mayang SariОценок пока нет
- Sas 20Документ4 страницыSas 20Sistine Rose LabajoОценок пока нет
- Respiratory SystemДокумент9 страницRespiratory Systemtheglobalnursing89% (9)
- The Language of Medicine - 9 - Chpt12exДокумент9 страницThe Language of Medicine - 9 - Chpt12exSalma LopezОценок пока нет
- Respiratory Disorders and PregnancyДокумент23 страницыRespiratory Disorders and PregnancyAngelie RojasОценок пока нет
- Criteria For MV WeaningДокумент7 страницCriteria For MV Weaning4g5xwdvh9sОценок пока нет
- Radiolucent in Chest X-RayДокумент64 страницыRadiolucent in Chest X-RaymunawasaОценок пока нет
- Breathing Techniques-A Review - 25 Different Types: October 2015Документ6 страницBreathing Techniques-A Review - 25 Different Types: October 2015Zahra SativaniОценок пока нет
- 1441-Article Text-4262-2-10-20200816Документ9 страниц1441-Article Text-4262-2-10-20200816MaimunahОценок пока нет
- Niv BK 9051941 EnusДокумент84 страницыNiv BK 9051941 EnusmatijahОценок пока нет
- Thorax and LungsДокумент64 страницыThorax and LungsGemmalene PaclebОценок пока нет
- Marquis Et Al 2023 CT Approach To Lung InjuryДокумент19 страницMarquis Et Al 2023 CT Approach To Lung InjuryMinh đăng ĐỗОценок пока нет
- 33.+ihtisyam,+231006 PublishДокумент7 страниц33.+ihtisyam,+231006 Publishvanessa300302Оценок пока нет
- C O P D: Hronic Bstructive Ulmonary IseaseДокумент53 страницыC O P D: Hronic Bstructive Ulmonary IseaseLe KhoaОценок пока нет
- Studi Faal Paru Dan Kebiasaan Merokok Pada Pekerja Yang Terpapar Debu Pada Perusahaan Konstruksi Di SurabayaДокумент10 страницStudi Faal Paru Dan Kebiasaan Merokok Pada Pekerja Yang Terpapar Debu Pada Perusahaan Konstruksi Di SurabayaNada LathifahОценок пока нет
- Medical Surgical Nursing Lab Oxygenation To Suctioning of Tracheostomy QuestionsДокумент6 страницMedical Surgical Nursing Lab Oxygenation To Suctioning of Tracheostomy Questionsclaire dimaano (colosus)Оценок пока нет
- 1 Ineffective Breathing PatternДокумент8 страниц1 Ineffective Breathing PatternNoel MontemayorОценок пока нет