Вам также может понравиться
- An Introduction To Medical Ethics: Dr. Philip S.L. Beh Email: Philipbeh@pathology - Hku.hkДокумент43 страницыAn Introduction To Medical Ethics: Dr. Philip S.L. Beh Email: Philipbeh@pathology - Hku.hksatyachakrabortyОценок пока нет
- Medical Law EthicsДокумент40 страницMedical Law EthicsAshutosh GuptaОценок пока нет
- Medical EthicsДокумент13 страницMedical EthicssatyachakrabortyОценок пока нет
- Medical Ethics: Introduction To Basic PrinciplesДокумент19 страницMedical Ethics: Introduction To Basic PrinciplessatyachakrabortyОценок пока нет
- Medical Ethics - ConceptsДокумент39 страницMedical Ethics - Conceptsjackie funtanillaОценок пока нет
- Deklarasi Helsinki PDFДокумент2 страницыDeklarasi Helsinki PDFnisa_neyshaaljufriОценок пока нет
- Deklarasi Helsinki PDFДокумент2 страницыDeklarasi Helsinki PDFnisa_neyshaaljufriОценок пока нет
- Handbook To Build An Hospital CRF PDFДокумент25 страницHandbook To Build An Hospital CRF PDFFernanda Ramírez100% (1)
- Lab Planning 09-12-21Документ1 страницаLab Planning 09-12-21satyachakrabortyОценок пока нет
- Downloadable Version E-BooksДокумент255 страницDownloadable Version E-BooksArun MozhiОценок пока нет
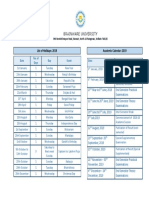
- Brainware University: List of Holidays: 2019 Academic Calendar: 2019Документ1 страницаBrainware University: List of Holidays: 2019 Academic Calendar: 2019satyachakrabortyОценок пока нет
- Disinfection in Hospitals: Dr.T.V.Rao MDДокумент71 страницаDisinfection in Hospitals: Dr.T.V.Rao MDsatyachakrabortyОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Seeker 1983 - Master Time FactorДокумент169 страницThe Seeker 1983 - Master Time FactorNarendra Kamma93% (15)
- REC Multiple Choice QuestionsДокумент2 страницыREC Multiple Choice QuestionsEnp Gus AgostoОценок пока нет
- DRHP Home First FinanceДокумент357 страницDRHP Home First FinanceHarsh KediaОценок пока нет
- LiveДокумент31 страницаLivebkaaljdaelvОценок пока нет
- F M Accounting - Lesson.1Документ58 страницF M Accounting - Lesson.1Versha ThakurОценок пока нет
- 06 BasicAccTP1 SantosДокумент3 страницы06 BasicAccTP1 SantosJohn Santos100% (1)
- Audit of Financial StatementsДокумент4 страницыAudit of Financial StatementsBrit NeyОценок пока нет
- GKEDC Open Letter To Pen Argyl Area ResidentsДокумент3 страницыGKEDC Open Letter To Pen Argyl Area ResidentsAnonymous arnc2g2N100% (1)
- Shirkah and Its Variant SummaryДокумент4 страницыShirkah and Its Variant SummaryOmayr QureshiОценок пока нет
- Feasibility Research On Rice Production For Zamboanga CooperativeДокумент40 страницFeasibility Research On Rice Production For Zamboanga Cooperativejeffrey ordonezОценок пока нет
- LN01 - Smart3075419 - 13 - FI - C07 - Analyzing Common StocksДокумент62 страницыLN01 - Smart3075419 - 13 - FI - C07 - Analyzing Common StocksNhung HồngОценок пока нет
- Cffinals PDFДокумент82 страницыCffinals PDFsultaniiuОценок пока нет
- Cma Tata MotorsДокумент25 страницCma Tata MotorsArchana MishraОценок пока нет
- CCVF BrochureДокумент35 страницCCVF BrochurekamalchakilamОценок пока нет
- INDIAN RAILWAYS - Source of Finance BudgetaryДокумент12 страницINDIAN RAILWAYS - Source of Finance Budgetaryjeya chandranОценок пока нет
- The Laws of Zakat - Session 1Документ15 страницThe Laws of Zakat - Session 1sayeed sayeedОценок пока нет
- Personal Finance 6th Edition Madura Solution ManualДокумент46 страницPersonal Finance 6th Edition Madura Solution Manualbrenda100% (22)
- State Governments Incentives For InvestorsДокумент6 страницState Governments Incentives For InvestorsbalqueesОценок пока нет
- Should Ice HospitalДокумент37 страницShould Ice HospitalPrasad Yadav100% (1)
- Corporate Valuation - 16th October 2021Документ2 страницыCorporate Valuation - 16th October 2021Shivam ChoudharyОценок пока нет
- SyllabusДокумент11 страницSyllabusMuhammad Qaisar LatifОценок пока нет
- Finance Lesson 3Документ7 страницFinance Lesson 3mhussainОценок пока нет
- Financial Accounting: Accounting Basics: Branches of AccountingДокумент7 страницFinancial Accounting: Accounting Basics: Branches of AccountingLucky HartanОценок пока нет
- A Stakeholder-Unifying, Cocreation Philosophy of MarketingДокумент6 страницA Stakeholder-Unifying, Cocreation Philosophy of MarketingKarnYoОценок пока нет
- Fin 201 Term Paper (Group L)Документ33 страницыFin 201 Term Paper (Group L)omarsakib19984Оценок пока нет
- Camels RatingДокумент12 страницCamels RatingImtiaz AhmedОценок пока нет
- M3 PJM1204 - BusinessAnalysis P2 Fall 2022Документ59 страницM3 PJM1204 - BusinessAnalysis P2 Fall 2022Kedze BaronОценок пока нет
- Fabm2 - Q2 - M1Документ17 страницFabm2 - Q2 - M1Gringo Rait100% (2)
- BBF 052716 816 PDFДокумент9 страницBBF 052716 816 PDFzpmellaОценок пока нет