Вам также может понравиться
- Food and Water Borne Diseases RUДокумент13 страницFood and Water Borne Diseases RUchariz bulaybulayОценок пока нет
- G8 Health 3.1Документ14 страницG8 Health 3.1Rhienzane L. MarasiganОценок пока нет
- HTP-Bed BathingДокумент3 страницыHTP-Bed BathingJoanna :DОценок пока нет
- 06 HEALTH TALK ImmunizationДокумент18 страниц06 HEALTH TALK Immunizationamit100% (3)
- Alternative Methods of BirthДокумент8 страницAlternative Methods of BirthDn CredibleОценок пока нет
- Pest Control and Methods of DishwashingДокумент43 страницыPest Control and Methods of DishwashingAnnieCastilloSampayanОценок пока нет
- Antenatal Examination DemonstrationДокумент10 страницAntenatal Examination DemonstrationSamarpit Singh0% (1)
- Illness Prevention Activities Are Designed To HelpДокумент2 страницыIllness Prevention Activities Are Designed To HelpAlleya SheeneОценок пока нет
- Proper Nutrition Instructional DesignДокумент5 страницProper Nutrition Instructional DesignChristine HernandezОценок пока нет
- Immunization EducationДокумент18 страницImmunization Educationamit92% (26)
- Fundamental of Nursing CA 1Документ2 страницыFundamental of Nursing CA 1BeltineОценок пока нет
- Health Maintenance of InfantДокумент59 страницHealth Maintenance of InfantMohamed Na3eemОценок пока нет
- ImmunizationДокумент29 страницImmunizationsuper coolОценок пока нет
- Abarracoso F. - TFN - Ass3Документ3 страницыAbarracoso F. - TFN - Ass3floramay.abarracosoОценок пока нет
- Lesson 6 - Prevention of IllnessДокумент1 страницаLesson 6 - Prevention of IllnessJlou VillartaОценок пока нет
- Jomarie padernal (2)Документ1 страницаJomarie padernal (2)2ndyearacc05Оценок пока нет
- Emilio Aguinaldo College: School of NursingДокумент2 страницыEmilio Aguinaldo College: School of NursingThe Mortal HowlerОценок пока нет
- Health Education About Immunization: College of Nursing Madurai Medical College MaduraiДокумент29 страницHealth Education About Immunization: College of Nursing Madurai Medical College Maduraijayashreeselvaraj100% (4)
- Syllabus NCM 109 Care of Mother Child Adolescent at Risk or With ProblemДокумент37 страницSyllabus NCM 109 Care of Mother Child Adolescent at Risk or With Problembrilliant dumay100% (1)
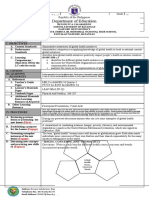
- Lesson ExemplarДокумент2 страницыLesson ExemplarAlvin LisondraОценок пока нет
- 3145-Article Text-27829-1-10-20210525Документ9 страниц3145-Article Text-27829-1-10-20210525Jewel Jeandy Ann TaojoОценок пока нет
- Bacud, Parick Jayson C.Документ4 страницыBacud, Parick Jayson C.Patrick Jayson BacudОценок пока нет
- Local Media5472392252259198951Документ7 страницLocal Media5472392252259198951Ralph Elvin MacanlalayОценок пока нет
- Imci Components of IMCI StrategyДокумент12 страницImci Components of IMCI StrategyPebbles PangilinanОценок пока нет
- Naskah Publikasi NUR BINTOROДокумент9 страницNaskah Publikasi NUR BINTOROnur bintoroОценок пока нет
- 2022 ACR Mam Luz DRRMДокумент4 страницы2022 ACR Mam Luz DRRMceleste c. casinilloОценок пока нет
- Midterm Comp. FPДокумент2 страницыMidterm Comp. FPSAEEDA ALMUQAHWIОценок пока нет
- CHN CS 5 PHC Services in OmanДокумент62 страницыCHN CS 5 PHC Services in OmanMelita Sheela AlvaОценок пока нет
- Edfd 459 - Portfolio PLC Health LessonsДокумент15 страницEdfd 459 - Portfolio PLC Health Lessonsapi-550981792Оценок пока нет
- Health Education - Finals - Demain - BlockBДокумент3 страницыHealth Education - Finals - Demain - BlockBJoshua DemainОценок пока нет
- CphparacourseДокумент3 страницыCphparacourseFRANZ LOUI KENDRICK BUGARINОценок пока нет
- Community Health NursingДокумент2 страницыCommunity Health NursingLordson Gem P. IbonОценок пока нет
- Food Hygiene and GMP Training WorkshopДокумент2 страницыFood Hygiene and GMP Training WorkshopMaricel BaltazarОценок пока нет
- Q3-Health-D3 CotДокумент4 страницыQ3-Health-D3 CotDennis MartinezОценок пока нет
- PPS Telemedicine Manual Jan 2021Документ36 страницPPS Telemedicine Manual Jan 2021Patricia Bernadette PalenciaОценок пока нет
- Workplace Hygiene EmployeesДокумент1 страницаWorkplace Hygiene EmployeesLorraine N MangenaОценок пока нет
- Elp Health 3Документ9 страницElp Health 3Charito Vargas CordialОценок пока нет
- Reflective Journal (HDU)Документ2 страницыReflective Journal (HDU)Wench Ryechelle SodosoОценок пока нет
- Community Health Nursing Project in Barangay La OpinionДокумент5 страницCommunity Health Nursing Project in Barangay La OpinionKathlyn PactorananОценок пока нет
- Anti-Asthma: PharmacologyДокумент6 страницAnti-Asthma: PharmacologyKyle De Sagun OtedaОценок пока нет
- Preventive Pediatric Care EssentialsДокумент7 страницPreventive Pediatric Care EssentialsCarla Elize DerainОценок пока нет
- Health Detailed Lesson PlanДокумент7 страницHealth Detailed Lesson PlanBREVISH DAME FRANCO100% (4)
- Periodontal Vaccines - A ReviewДокумент4 страницыPeriodontal Vaccines - A ReviewdocrkОценок пока нет
- Chn211rle Epi Group1Документ24 страницыChn211rle Epi Group1Alex Antiporda100% (3)
- Widdoes ST., Brgy. II, City of San Fernando, La Union 2500 PhilippinesДокумент7 страницWiddoes ST., Brgy. II, City of San Fernando, La Union 2500 Philippinesricky torresОценок пока нет
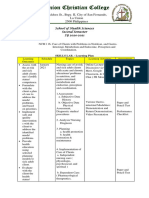
- Safe Healthy LecДокумент9 страницSafe Healthy LecMackoy LoganОценок пока нет
- DLL Mapeh-3 Q2 W9Документ2 страницыDLL Mapeh-3 Q2 W9Marita bagaslaoОценок пока нет
- 3.artikel JKM Vol 12 No 2 Tahun 2019 Alowadodo Harefa Tengku Muhammad Fauzi Juli Jamnasi 14 18Документ5 страниц3.artikel JKM Vol 12 No 2 Tahun 2019 Alowadodo Harefa Tengku Muhammad Fauzi Juli Jamnasi 14 18Chika AmaliaОценок пока нет
- Early Childhood Caries: International Journal of Dentistry October 2011Документ8 страницEarly Childhood Caries: International Journal of Dentistry October 2011Latiefah NWОценок пока нет
- Nursing Management of Reproductive DrugsДокумент5 страницNursing Management of Reproductive DrugsKathleen AngОценок пока нет
- Interns trainingДокумент4 страницыInterns trainingAlemsegedОценок пока нет
- MSN Activity 3Документ2 страницыMSN Activity 3Pamela Loyola NuestroОценок пока нет
- MARY GRACE (CHN) Final Presentation For FNCPДокумент6 страницMARY GRACE (CHN) Final Presentation For FNCPMary grace VirayОценок пока нет
- Effects of Safety Food Handling Practices Among Senior High School Students in Celtech CollegДокумент42 страницыEffects of Safety Food Handling Practices Among Senior High School Students in Celtech CollegMa Andrea100% (1)
- Infection Control and Prevention in DentistryДокумент7 страницInfection Control and Prevention in DentistryHiba HamidОценок пока нет
- Importance of Modern MicrobiologyДокумент1 страницаImportance of Modern MicrobiologyMhel Rose BenitezОценок пока нет
- IMCI skills lab focuses on childhood illnessesДокумент11 страницIMCI skills lab focuses on childhood illnessesivy annОценок пока нет
- Lesson Plan On Prevention of MalnutritionДокумент7 страницLesson Plan On Prevention of MalnutritionPriyanka NilewarОценок пока нет
- Online Activity 5 11 2020 15Документ2 страницыOnline Activity 5 11 2020 15kyle otedaОценок пока нет
- Basic Foreign Language (Japanese) Activity 2Документ1 страницаBasic Foreign Language (Japanese) Activity 2Kyle De Sagun OtedaОценок пока нет
- Hypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenДокумент37 страницHypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenKyle De Sagun OtedaОценок пока нет
- Thyroid Medications: PharmacologyДокумент2 страницыThyroid Medications: PharmacologyKyle De Sagun OtedaОценок пока нет
- Hyperchloremia: Group 11 Singh, Joshua Silverio, Silver John Tabarnilla, Michiko Unico, Paula Villa, JustinaДокумент15 страницHyperchloremia: Group 11 Singh, Joshua Silverio, Silver John Tabarnilla, Michiko Unico, Paula Villa, JustinaKyle De Sagun OtedaОценок пока нет
- Anti-Asthma: PharmacologyДокумент6 страницAnti-Asthma: PharmacologyKyle De Sagun OtedaОценок пока нет
- Hypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenДокумент37 страницHypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenKyle De Sagun OtedaОценок пока нет
- Hiragana Writing Practice SheetsДокумент10 страницHiragana Writing Practice SheetsDina Dinel100% (2)
- Hypokalemia: Presented By: Group 4 Dolfo, Dominise, Ejercito, FloraldeДокумент20 страницHypokalemia: Presented By: Group 4 Dolfo, Dominise, Ejercito, FloraldeKyle De Sagun OtedaОценок пока нет
- Hypermagnesemia: Lim - Madalan - Madelo - MagalitДокумент17 страницHypermagnesemia: Lim - Madalan - Madelo - MagalitKyle De Sagun Oteda100% (1)
- Group 3 HyperkalemiaДокумент23 страницыGroup 3 HyperkalemiaKyle De Sagun OtedaОценок пока нет
- Hypernatremia G1 2Документ14 страницHypernatremia G1 2Kyle De Sagun OtedaОценок пока нет
- Copd Drugs: PharmacologyДокумент3 страницыCopd Drugs: PharmacologyKyle De Sagun OtedaОценок пока нет
- Antihypertensives: PharmacologyДокумент4 страницыAntihypertensives: PharmacologyKyle De Sagun OtedaОценок пока нет
- Editorial Cartoon About COVID-19 (Nursing Informatics) : Jerome Brickster C. Salud Andrew Angelo O. Lim Jan Kyle S. OtedaДокумент3 страницыEditorial Cartoon About COVID-19 (Nursing Informatics) : Jerome Brickster C. Salud Andrew Angelo O. Lim Jan Kyle S. OtedaKyle De Sagun OtedaОценок пока нет
- New Text DocumentДокумент1 страницаNew Text DocumentKyle De Sagun OtedaОценок пока нет
- INFOДокумент6 страницINFOKyle De Sagun OtedaОценок пока нет
- Pharmacology: AntacidsДокумент3 страницыPharmacology: AntacidsKyle De Sagun OtedaОценок пока нет
- Drug Study OtedaaДокумент22 страницыDrug Study OtedaaKyle De Sagun OtedaОценок пока нет
- Drug StudyДокумент8 страницDrug StudyKyle De Sagun OtedaОценок пока нет
- Drug Study Sa PharmaДокумент4 страницыDrug Study Sa PharmaKyle De Sagun Oteda100% (1)
- Nursing Care of Clients With Pregnancy-Induced HypertensionДокумент3 страницыNursing Care of Clients With Pregnancy-Induced HypertensionKyle De Sagun OtedaОценок пока нет
- ANTIVIRALS OtedaДокумент2 страницыANTIVIRALS OtedaKyle De Sagun OtedaОценок пока нет
- Ncm-Quiz-Rle - OtedaДокумент2 страницыNcm-Quiz-Rle - OtedaKyle De Sagun OtedaОценок пока нет
- Drug Study Ni DeanДокумент6 страницDrug Study Ni DeanKyle De Sagun OtedaОценок пока нет
- ANTIVIRALS OtedaДокумент2 страницыANTIVIRALS OtedaKyle De Sagun OtedaОценок пока нет
- Nursing Care Plan (Maternal Rle) : Emilio Aguinaldo CollegeДокумент9 страницNursing Care Plan (Maternal Rle) : Emilio Aguinaldo CollegeKyle De Sagun Oteda100% (2)
- BIOETHICS by OTEDAДокумент5 страницBIOETHICS by OTEDAKyle De Sagun OtedaОценок пока нет
- BIOETHICS by OTEDAДокумент5 страницBIOETHICS by OTEDAKyle De Sagun OtedaОценок пока нет
- ANTIVIRALS OtedaДокумент2 страницыANTIVIRALS OtedaKyle De Sagun OtedaОценок пока нет
- Endodontics DiagnosisДокумент6 страницEndodontics DiagnosisRPОценок пока нет
- Endodontic Surgery: Incision and DrainageДокумент8 страницEndodontic Surgery: Incision and DrainageHadoo OolaОценок пока нет
- Using Growth Charts to Monitor Child NutritionДокумент13 страницUsing Growth Charts to Monitor Child Nutritionp1843dОценок пока нет
- What Is Ehlers-Danlos Syndrome?: Joint HypermobilityДокумент4 страницыWhat Is Ehlers-Danlos Syndrome?: Joint HypermobilityisisjadidОценок пока нет
- SEO-optimized title for Vietnamese high school graduation exam paperДокумент8 страницSEO-optimized title for Vietnamese high school graduation exam paperTrang Đỗ100% (3)
- Hymenolepis Diminuta (Rodolphi, 1819) Infection in A Child FromДокумент2 страницыHymenolepis Diminuta (Rodolphi, 1819) Infection in A Child Frommuhammad nurhadiОценок пока нет
- Cystoscopy 508Документ6 страницCystoscopy 508Jayakumar D SwamyОценок пока нет
- Bordetella: Bordetella Organisms Are Small, Gram-Negative Coccobacilli Which Are Strict Aerobes. The ThreeДокумент7 страницBordetella: Bordetella Organisms Are Small, Gram-Negative Coccobacilli Which Are Strict Aerobes. The ThreeFlor OMОценок пока нет
- Skin DiseasesДокумент33 страницыSkin DiseasesKir Kal KarОценок пока нет
- Journal of The California Dental Association Oct 2007Документ70 страницJournal of The California Dental Association Oct 2007gerardo_ureñaОценок пока нет
- General Education Set 15Документ9 страницGeneral Education Set 15jenalynОценок пока нет
- Review of The Systems: Dr. Made Ratna Saraswati, SPPD Wednesday, 13 Oct 2010Документ22 страницыReview of The Systems: Dr. Made Ratna Saraswati, SPPD Wednesday, 13 Oct 2010Riska ApriliaОценок пока нет
- Prelim Risk Management Apply To Safety SecurityДокумент16 страницPrelim Risk Management Apply To Safety SecurityDENNIS T. BALANGUEОценок пока нет
- Community Health Nursing Course OutlineДокумент5 страницCommunity Health Nursing Course OutlineMeeKo VideñaОценок пока нет
- Dengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Документ9 страницDengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Abdul Shakur FaisalОценок пока нет
- Coronavirus ThesisДокумент4 страницыCoronavirus Thesisdnr68wp2100% (2)
- Reference Team R001 - Summary of PleadingsДокумент5 страницReference Team R001 - Summary of PleadingsMeAnn TumbagaОценок пока нет
- Ebp PosterДокумент1 страницаEbp Posterapi-340595961Оценок пока нет
- Parasitology Guide Questions 1Документ2 страницыParasitology Guide Questions 1Cess LacatangoОценок пока нет
- Poultry DiseasesДокумент12 страницPoultry DiseasesHassanQadeer67% (3)
- Bulletin - Diseases of Mud Crabs in India - InnerДокумент36 страницBulletin - Diseases of Mud Crabs in India - InnerDr. K.P.JithendranОценок пока нет
- Pharma SheetДокумент2 страницыPharma SheetcdctinОценок пока нет
- Module 2 Lesson 1 Activity - 2Документ2 страницыModule 2 Lesson 1 Activity - 2John Paul DapitanonОценок пока нет
- Psychological Impact of COVID-19 Pandemic in The PhilippinesДокумент23 страницыPsychological Impact of COVID-19 Pandemic in The PhilippinesArgonne Robert AblanqueОценок пока нет
- Occupational Health Form: General DetailsДокумент2 страницыOccupational Health Form: General DetailsKhushal khanОценок пока нет
- Masker Training for Covid-19 PreventionДокумент6 страницMasker Training for Covid-19 Preventionmuhammad zakiОценок пока нет
- WHO 2011 Typhoid FeverДокумент39 страницWHO 2011 Typhoid FeverVizzi Alvi Fitrah NasutionОценок пока нет
- Narrative of Dry Run SimulationДокумент2 страницыNarrative of Dry Run SimulationJhen SalamatОценок пока нет
- Communicative II, Unit 2 QuestionsДокумент2 страницыCommunicative II, Unit 2 QuestionsAddis VLOG100% (3)
- Orthopaedic Surgery MCQsДокумент23 страницыOrthopaedic Surgery MCQsWinifred Chen70% (10)