Вам также может понравиться
- PJMS 34 999 PDFДокумент5 страницPJMS 34 999 PDFdinda mentari putriОценок пока нет
- Jadwal Perawat Igd Bulan Mei 2021 RevisiДокумент7 страницJadwal Perawat Igd Bulan Mei 2021 Revisidinda mentari putriОценок пока нет
- DeskriptifДокумент71 страницаDeskriptifdinda mentari putriОценок пока нет
- Jadwal Perawat Igd Bulan April 2021 RevisiДокумент7 страницJadwal Perawat Igd Bulan April 2021 Revisidinda mentari putriОценок пока нет
- Dimensi SERVPERF PDFДокумент7 страницDimensi SERVPERF PDFdinda mentari putriОценок пока нет
- PJMS 34 999 PDFДокумент5 страницPJMS 34 999 PDFdinda mentari putriОценок пока нет
- Jurnal InternasionalДокумент9 страницJurnal Internasionaldinda mentari putriОценок пока нет
- Dimensi SERVPERF PDFДокумент7 страницDimensi SERVPERF PDFdinda mentari putriОценок пока нет
- Jurnal Internasional 13Документ9 страницJurnal Internasional 13dinda mentari putriОценок пока нет
- Jurnal Internasional 4Документ9 страницJurnal Internasional 4dinda mentari putriОценок пока нет
- Jurnal Internasional 5Документ16 страницJurnal Internasional 5dinda mentari putriОценок пока нет
- Jurnal Internasional 2Документ11 страницJurnal Internasional 2dinda mentari putriОценок пока нет
- Jurnal Internasional 3Документ12 страницJurnal Internasional 3dinda mentari putriОценок пока нет
- F 561Документ9 страницF 561Tarni AyuningsihОценок пока нет
- Jurnal Internasional 3Документ12 страницJurnal Internasional 3dinda mentari putriОценок пока нет
- Jurnal Internasional 10Документ9 страницJurnal Internasional 10dinda mentari putriОценок пока нет
- Jurnal Internasional 9Документ14 страницJurnal Internasional 9dinda mentari putriОценок пока нет
- Jurnal Internasional 13Документ9 страницJurnal Internasional 13dinda mentari putriОценок пока нет
- Jurnal Internasional 12Документ16 страницJurnal Internasional 12dinda mentari putriОценок пока нет
- Jurnal Internasional 11Документ12 страницJurnal Internasional 11dinda mentari putriОценок пока нет
- Jurnal Internasional Kualitas PelayananaДокумент6 страницJurnal Internasional Kualitas Pelayananadinda mentari putriОценок пока нет
- Jurnal Internasional 3Документ12 страницJurnal Internasional 3dinda mentari putriОценок пока нет
- Analysis of Factors Are Relating To Service Quality and Patient Loyalty atДокумент1 страницаAnalysis of Factors Are Relating To Service Quality and Patient Loyalty atdinda mentari putriОценок пока нет
- Jurnal Internasional 14Документ11 страницJurnal Internasional 14dinda mentari putriОценок пока нет
- Analysis of Factors Are Relating To Service Quality and Patient Loyalty atДокумент1 страницаAnalysis of Factors Are Relating To Service Quality and Patient Loyalty atdinda mentari putriОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
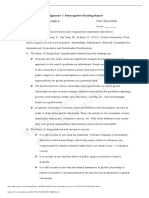
- How To Write A CritiqueДокумент4 страницыHow To Write A CritiqueSoc SaballaОценок пока нет
- Tale of A Dramatic Exit From The Cave Is The Source of True UnderstandingДокумент3 страницыTale of A Dramatic Exit From The Cave Is The Source of True UnderstandingIldjohn CarrilloОценок пока нет
- Michael Pidd DECISION MAKING Systems Modelling, Theory and Practice PDFДокумент222 страницыMichael Pidd DECISION MAKING Systems Modelling, Theory and Practice PDFmohimran2002100% (1)
- Anantrao Pawar College of Achitecture, Pune.: Analysis of Courtyard Space in Architectural InstituteДокумент8 страницAnantrao Pawar College of Achitecture, Pune.: Analysis of Courtyard Space in Architectural InstituteJayant Dhumal PatilОценок пока нет
- Higher Studies in USA (MS-PHD)Документ32 страницыHigher Studies in USA (MS-PHD)Graphic DesignerОценок пока нет
- Ronquillo A Nstp100 Am22 Tee2Документ3 страницыRonquillo A Nstp100 Am22 Tee2Angelo RonquilloОценок пока нет
- Sociological and Legal Bases of School - Community PartnershipsДокумент16 страницSociological and Legal Bases of School - Community PartnershipsAljun Emperado100% (17)
- Informative Speech Outline LatestДокумент4 страницыInformative Speech Outline LatestAzlan KinGshah II100% (2)
- Miguel L. Rojas-Sotelo, PHD Cultural Maps, Networks and Flows: The History and Impact of The Havana Biennale 1984 To The PresentДокумент562 страницыMiguel L. Rojas-Sotelo, PHD Cultural Maps, Networks and Flows: The History and Impact of The Havana Biennale 1984 To The PresentIsobel Whitelegg100% (1)
- Home Economics PDFДокумент29 страницHome Economics PDFalpha100% (2)
- Chapter 2 Answer SheetДокумент3 страницыChapter 2 Answer SheetsharjaОценок пока нет
- Essay For AdmissionДокумент1 страницаEssay For AdmissionValerii EssayОценок пока нет
- Digital Maturity Model: + 179 Specific Digital Criteria To Test Your Organizational MaturityДокумент1 страницаDigital Maturity Model: + 179 Specific Digital Criteria To Test Your Organizational MaturityDaiani Roberti100% (1)
- Student Engagement GuideBook 1.5 - 20210118Документ63 страницыStudent Engagement GuideBook 1.5 - 20210118jesicaОценок пока нет
- Carnival of The Animals Teachers ResourceДокумент39 страницCarnival of The Animals Teachers Resourceflute01100% (1)
- Traditional Chinese Medicine and Acupuncture in Ontario: Report To The Minister of Health and Long-Term CareДокумент22 страницыTraditional Chinese Medicine and Acupuncture in Ontario: Report To The Minister of Health and Long-Term CareRichard SiahaanОценок пока нет
- OO0523Документ16 страницOO0523Anonymous 9eadjPSJNgОценок пока нет
- Videbeck - Psychiatric Mental Health Nursing - NewДокумент27 страницVidebeck - Psychiatric Mental Health Nursing - NewJohnrey Tesoro0% (1)
- AP BOE-2017 NotificationsДокумент10 страницAP BOE-2017 NotificationsShashikant ChoudhariОценок пока нет
- Rizal Street, Poblacion, Muntinlupa City Telefax:8828-8037Документ14 страницRizal Street, Poblacion, Muntinlupa City Telefax:8828-8037Marilou KimayongОценок пока нет
- USMLE StepДокумент1 страницаUSMLE StepAscend KannanОценок пока нет
- Bee PPT Sem 2Документ14 страницBee PPT Sem 2Divya ZopeОценок пока нет
- Per. 1 - Cold War - Exit TicketДокумент6 страницPer. 1 - Cold War - Exit TicketB ReyОценок пока нет
- ĐỀ THAM KHẢO SỐ 1Документ6 страницĐỀ THAM KHẢO SỐ 1Lê Hồng LoanОценок пока нет
- 0 - Shruti Chakranarayn CVДокумент5 страниц0 - Shruti Chakranarayn CVShruti AmritwarОценок пока нет
- 4024 Mathematics (Syllabus D) : MARK SCHEME For The May/June 2011 Question Paper For The Guidance of TeachersДокумент4 страницы4024 Mathematics (Syllabus D) : MARK SCHEME For The May/June 2011 Question Paper For The Guidance of TeachersAyra MujibОценок пока нет
- This Study Resource Was: Public Support To Active Participation. Amsterdam, Netherlands: National Committee ForДокумент3 страницыThis Study Resource Was: Public Support To Active Participation. Amsterdam, Netherlands: National Committee ForJoel Christian HernalinОценок пока нет
- Math 10-Q1-M9Документ14 страницMath 10-Q1-M9Ainee Grace DolleteОценок пока нет
- Evidence-Based Treatment of Attention Deficit/ Hyperactivity Disorder in A Preschool-Age Child: A Case StudyДокумент10 страницEvidence-Based Treatment of Attention Deficit/ Hyperactivity Disorder in A Preschool-Age Child: A Case StudyCristinaОценок пока нет
- Comprehension (Indicators, Levels, Skills, Activity)Документ31 страницаComprehension (Indicators, Levels, Skills, Activity)Angel Dixcee Lapugot AguilanОценок пока нет