Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Improving Functional Outcomes in Physical Rehabilitation 2nd Edition Ebook PDFДокумент62 страницыImproving Functional Outcomes in Physical Rehabilitation 2nd Edition Ebook PDFgeorge.leon963100% (46)
- Anxiety Experiences of SHS Students On Our Lady of Fatima University On Test Performance and Self-EsteemДокумент22 страницыAnxiety Experiences of SHS Students On Our Lady of Fatima University On Test Performance and Self-EsteemVictor TibayanОценок пока нет
- Lesson Plan Panel DiscussionДокумент9 страницLesson Plan Panel DiscussionAwasthi KovidОценок пока нет
- Topic 1 Introduction To Guidance and CounsellingДокумент14 страницTopic 1 Introduction To Guidance and CounsellingNanthiniNaveesha0% (2)
- The Study of Primary Psychotic Disorders With Concurrent Substance Abuse in Terms of Their Diagnostic StabilityДокумент12 страницThe Study of Primary Psychotic Disorders With Concurrent Substance Abuse in Terms of Their Diagnostic StabilitySynthiaОценок пока нет
- Anatomy of The BrainДокумент38 страницAnatomy of The BrainnayanaОценок пока нет
- The Betari BoxДокумент6 страницThe Betari BoxAmisaha0% (1)
- RRLДокумент3 страницыRRLJiffy Roseveery CervantesОценок пока нет
- Peace of Mind Academic Motivation and Academic Achievement in Filipino High School StudentsДокумент8 страницPeace of Mind Academic Motivation and Academic Achievement in Filipino High School Studentsjazzy umbalОценок пока нет
- HolandaДокумент11 страницHolandaAlvaro Bejarano MartinОценок пока нет
- GCSE Psychology Topic A How Do We See Our World?Документ28 страницGCSE Psychology Topic A How Do We See Our World?Ringo ChuОценок пока нет
- Learning TargetsДокумент1 страницаLearning TargetsCarlos Leo SantosОценок пока нет
- The Minds of Machines - Issue 87 - Philosophy NowДокумент4 страницыThe Minds of Machines - Issue 87 - Philosophy NowVovan VovanОценок пока нет
- Teddy BearДокумент6 страницTeddy BearPâmela MuchaОценок пока нет
- Schizoaffective Disorder in The DSM 5 PDFДокумент5 страницSchizoaffective Disorder in The DSM 5 PDFpipiitopandabamboo247Оценок пока нет
- The Science Behind Reading Genius - 3-10-06Документ35 страницThe Science Behind Reading Genius - 3-10-06Deanna Jones100% (10)
- BET 4108-Educational Technology - CAT 1 and 2Документ6 страницBET 4108-Educational Technology - CAT 1 and 2Elias BonkeОценок пока нет
- Respirology Adult Sample Polysomnography Report eДокумент2 страницыRespirology Adult Sample Polysomnography Report eignatiaratna prativiОценок пока нет
- Consumer Socialization of ChildrenДокумент32 страницыConsumer Socialization of ChildrenKristóf Bence SzabóОценок пока нет
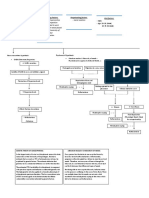
- Predisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsДокумент3 страницыPredisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsRein TamayoОценок пока нет
- 2015 - The Evolution of Behaviour Therapy and Cognitive Behaviour Therapy - RachmanДокумент8 страниц2015 - The Evolution of Behaviour Therapy and Cognitive Behaviour Therapy - RachmanFabián MaeroОценок пока нет
- NCP For BipolarДокумент11 страницNCP For BipolarFatima Medriza DuranОценок пока нет
- Curs 2-Managementul Pacientului Cu TCCДокумент46 страницCurs 2-Managementul Pacientului Cu TCCMarina ApostolОценок пока нет
- Folkman, Moskowitz (2000) Stress, Positive Emotion, CopingДокумент4 страницыFolkman, Moskowitz (2000) Stress, Positive Emotion, CopingDavid Fernando MorenoОценок пока нет
- Biopsy Practice TestДокумент37 страницBiopsy Practice TestMG SarabosingОценок пока нет
- Neuroanatomy ReviewДокумент107 страницNeuroanatomy ReviewAlan Magpantay100% (1)
- Antipsychotic Drugs Chapter 29Документ15 страницAntipsychotic Drugs Chapter 29jemms16Оценок пока нет
- Understanding Psycho Pa To LogyДокумент8 страницUnderstanding Psycho Pa To LogynicecoolemmaОценок пока нет
- Positive Coping Strategies For College Students Under StressДокумент27 страницPositive Coping Strategies For College Students Under Stressapi-402807267Оценок пока нет
- Essay (Revised)Документ6 страницEssay (Revised)Lorie Mae DomingoОценок пока нет