Вам также может понравиться
- Old-School Essentials Adventure Anthology 2 v0-3Документ38 страницOld-School Essentials Adventure Anthology 2 v0-3Μιχάλης Τερζάκης0% (2)
- Reference BookletДокумент35 страницReference BookletΜιχάλης Τερζάκης57% (7)
- Old-School Essentials Adventure Anthology 1 v0-4Документ44 страницыOld-School Essentials Adventure Anthology 1 v0-4Μιχάλης Τερζάκης20% (5)
- OSE Random Gear - FUNNEL GEARДокумент1 страницаOSE Random Gear - FUNNEL GEARΜιχάλης ΤερζάκηςОценок пока нет
- OSE The Pelietic ChurchДокумент3 страницыOSE The Pelietic ChurchΜιχάλης ΤερζάκηςОценок пока нет
- Illmire Pre-Gen CharДокумент7 страницIllmire Pre-Gen CharΜιχάλης ΤερζάκηςОценок пока нет
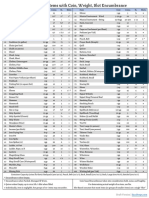
- Item Cost Coins Lb. Slots Item Cost Coins Lb. Slots: Draft VersionДокумент1 страницаItem Cost Coins Lb. Slots Item Cost Coins Lb. Slots: Draft VersionΜιχάλης ΤερζάκηςОценок пока нет
- Origins of PHC and SPHCДокумент11 страницOrigins of PHC and SPHCΜιχάλης ΤερζάκηςОценок пока нет
- Gauld Et Al WHR 2008 PHC Policy How Wide Is The Gap Between Agenta and Implementation 12 High IncomeДокумент21 страницаGauld Et Al WHR 2008 PHC Policy How Wide Is The Gap Between Agenta and Implementation 12 High IncomeΜιχάλης ΤερζάκηςОценок пока нет
- Tangled (Pages) (OSE)Документ24 страницыTangled (Pages) (OSE)Μιχάλης Τερζάκης50% (8)
- Social Epidimiology - HistoryДокумент7 страницSocial Epidimiology - HistoryΜιχάλης ΤερζάκηςОценок пока нет
- Difference SPHC Vs CPHCДокумент9 страницDifference SPHC Vs CPHCΜιχάλης ΤερζάκηςОценок пока нет
- Crypts of Kelemvor 5eДокумент15 страницCrypts of Kelemvor 5eΜιχάλης ΤερζάκηςОценок пока нет
- Hikvision Fever Screening Thermal CameraДокумент1 страницаHikvision Fever Screening Thermal CameraΜιχάλης ΤερζάκηςОценок пока нет
- The Dolmenwood CalendarДокумент22 страницыThe Dolmenwood CalendarΜιχάλης Τερζάκης100% (1)
- Dolmenwood House Rules (NGP) (Basic, BX)Документ1 страницаDolmenwood House Rules (NGP) (Basic, BX)Μιχάλης Τερζάκης0% (1)
- Dolmenwood Hex Crawl ProcedureДокумент2 страницыDolmenwood Hex Crawl ProcedureΜιχάλης Τερζάκης100% (2)
- Stonehell Dungeon, Lost Level (LL)Документ8 страницStonehell Dungeon, Lost Level (LL)Μιχάλης ΤερζάκηςОценок пока нет
- The Isle of Forgotten Gods (Basic, BX)Документ38 страницThe Isle of Forgotten Gods (Basic, BX)Μιχάλης Τερζάκης100% (1)
- DRA12 - The Barber of Silverymoon PDFДокумент13 страницDRA12 - The Barber of Silverymoon PDFlordejulioОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Watch One Piece English SubDub Online Free On Zoro - ToДокумент1 страницаWatch One Piece English SubDub Online Free On Zoro - ToSadeusuОценок пока нет
- Uh 60 ManualДокумент241 страницаUh 60 ManualAnonymous ddjwf1dqpОценок пока нет
- CH 15Документ58 страницCH 15Chala1989Оценок пока нет
- EmployWise JAVA ASSIGNMENTДокумент2 страницыEmployWise JAVA ASSIGNMENTPreet PatelОценок пока нет
- Personal Narrative RevisedДокумент3 страницыPersonal Narrative Revisedapi-549224109Оценок пока нет
- The Serious Student of HistoryДокумент5 страницThe Serious Student of HistoryCrisanto King CortezОценок пока нет
- Fluoride - Wide Range of Serious Health Problems"Документ29 страницFluoride - Wide Range of Serious Health Problems"zataullah100% (2)
- June 2014 (v3) QP - Paper 3 CIE Physics IGCSEДокумент20 страницJune 2014 (v3) QP - Paper 3 CIE Physics IGCSECole KhantОценок пока нет
- Guidelines For Plenipotentiary - 1Документ6 страницGuidelines For Plenipotentiary - 1Oladimeji Ibukun IjaodolaОценок пока нет
- Rab Sikda Optima 2016Документ20 страницRab Sikda Optima 2016Julius Chatry UniwalyОценок пока нет
- FHHR 013 Red Tag Procedure PDFДокумент5 страницFHHR 013 Red Tag Procedure PDFN3N5YОценок пока нет
- Needle BasicsДокумент31 страницаNeedle BasicsARYAN RATHOREОценок пока нет
- Gmail - ICICI BANK I PROCESS HIRING FOR BACKEND - OPERATION PDFДокумент2 страницыGmail - ICICI BANK I PROCESS HIRING FOR BACKEND - OPERATION PDFDeepankar ChoudhuryОценок пока нет
- SAED90DR Rev1 2 21.01.2011Документ24 страницыSAED90DR Rev1 2 21.01.2011Cherry AbhiОценок пока нет
- What Is A Fired Heater in A RefineryДокумент53 страницыWhat Is A Fired Heater in A RefineryCelestine OzokechiОценок пока нет
- Friday 25 Mar 12:15 AM Friday 25 Mar 5:30 AM: Emirates CGK DXBДокумент3 страницыFriday 25 Mar 12:15 AM Friday 25 Mar 5:30 AM: Emirates CGK DXBDONI ARTAОценок пока нет
- ProjectДокумент33 страницыProjectPiyush PatelОценок пока нет
- Mobile Services: Your Account Summary This Month'S ChargesДокумент3 страницыMobile Services: Your Account Summary This Month'S Chargeskumarvaibhav301745Оценок пока нет
- Chapter 24 - The Solar SystemДокумент36 страницChapter 24 - The Solar SystemHeather Blackwell100% (1)
- VLSI Implementation of Floating Point AdderДокумент46 страницVLSI Implementation of Floating Point AdderParamesh Waran100% (1)
- English 2nd Quarter Week 7 Connotation DenotationДокумент28 страницEnglish 2nd Quarter Week 7 Connotation DenotationEdward Estrella GuceОценок пока нет
- Abbas Ali Mandviwala 200640147: Ba1530: Information Systems and Organization StudiesДокумент11 страницAbbas Ali Mandviwala 200640147: Ba1530: Information Systems and Organization Studiesshayan sohailОценок пока нет
- TAC42055 - HO01 Edition I2.0: Section 1 Module 1 Page 1Документ69 страницTAC42055 - HO01 Edition I2.0: Section 1 Module 1 Page 1matheus santosОценок пока нет
- English For General SciencesДокумент47 страницEnglish For General Sciencesfauzan ramadhanОценок пока нет
- What Are Some of The Best Books On Computer ScienceДокумент9 страницWhat Are Some of The Best Books On Computer ScienceSarthak ShahОценок пока нет
- Process Industry Practices Insulation: PIP INEG2000 Guidelines For Use of Insulation PracticesДокумент15 страницProcess Industry Practices Insulation: PIP INEG2000 Guidelines For Use of Insulation PracticesZubair RaoofОценок пока нет
- Atom SDДокумент5 страницAtom SDatomsa shiferaОценок пока нет
- RESEARCH 10 Module 1 Lesson 1 (WEEK 1-2)Документ5 страницRESEARCH 10 Module 1 Lesson 1 (WEEK 1-2)DennisОценок пока нет
- Marieb ch3dДокумент20 страницMarieb ch3dapi-229554503Оценок пока нет
- Lifting PermanentmagnetДокумент6 страницLifting PermanentmagnetShekh Muhsen Uddin Ahmed100% (1)