Вам также может понравиться
- Nursing Care PlanДокумент12 страницNursing Care Plankeishaaa29100% (6)
- NCP Acute PainДокумент3 страницыNCP Acute PainDyanne BОценок пока нет
- Case: Liver Cirrhosis Assessment:: Nursing InferenceДокумент7 страницCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirОценок пока нет
- Self Care DeficitДокумент4 страницыSelf Care DeficitEllaine RamirezОценок пока нет
- Nursing Care PlanДокумент4 страницыNursing Care PlanJoy Callo100% (2)
- NCP FVDДокумент2 страницыNCP FVDMarlon AnryОценок пока нет
- NCP Pre EclampsiaДокумент2 страницыNCP Pre EclampsiaFarrah Grace Birowa0% (1)
- NCP - Deficient Fluid VolumeДокумент2 страницыNCP - Deficient Fluid VolumerobbychuaОценок пока нет
- NCP LocДокумент2 страницыNCP LocMel RodolfoОценок пока нет
- CP Intestinal Obstruction Nursing Care PlanДокумент7 страницCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaОценок пока нет
- Subjective: Long Term: Independent:: Iloilo Doctors' College College of NursingДокумент5 страницSubjective: Long Term: Independent:: Iloilo Doctors' College College of NursingAbie Jean Balbontin100% (1)
- NCP PancreatitisДокумент2 страницыNCP PancreatitisJeanelle Generoso100% (1)
- NCP Acute PancreatitisДокумент4 страницыNCP Acute PancreatitisJamil Lorca94% (17)
- Thyroidectomy NCPДокумент1 страницаThyroidectomy NCPkzbreakerrОценок пока нет
- NCP - Patient With Endotracheal TubeДокумент1 страницаNCP - Patient With Endotracheal TubeSelwynVillamorPatenteОценок пока нет
- Nursing Care PlanДокумент5 страницNursing Care Planruggero07100% (2)
- NCP Set 1Документ18 страницNCP Set 1Augene Toribio50% (2)
- Gallstone NCPДокумент2 страницыGallstone NCPKelly RiedingerОценок пока нет
- Flank Pain, Anxiety...Документ7 страницFlank Pain, Anxiety...reneighdОценок пока нет
- Gout N C P BY BHERU LALДокумент1 страницаGout N C P BY BHERU LALBheru LalОценок пока нет
- Assessment Diagnosis Planning Intervention Rationale EvaluationДокумент11 страницAssessment Diagnosis Planning Intervention Rationale EvaluationDeo OlarteОценок пока нет
- Nanda NCP BasedДокумент14 страницNanda NCP Baseddeliejoyce100% (1)
- Nursing Care Plan 1 DiagДокумент4 страницыNursing Care Plan 1 Diagguysornngam100% (1)
- Hypertension Nursing Care PlanДокумент3 страницыHypertension Nursing Care PlanAsylla PajijiОценок пока нет
- NCP GbsДокумент2 страницыNCP GbsJaylord VerazonОценок пока нет
- Deficit)Документ2 страницыDeficit)Lee DeeОценок пока нет
- Assessment Explanation Planning Interventions Rationale Evaluation Subjective: Objective: STG: STGДокумент11 страницAssessment Explanation Planning Interventions Rationale Evaluation Subjective: Objective: STG: STGGrape JuiceОценок пока нет
- NCP Knowledge DeficitДокумент1 страницаNCP Knowledge Deficittspears82100% (2)
- Acute Renal Failure Nursing Care PlanДокумент4 страницыAcute Renal Failure Nursing Care PlanKrisianne Mae Lorenzo Francisco80% (5)
- Carpenito-Moyet, L. J. (2009) : IndependentДокумент3 страницыCarpenito-Moyet, L. J. (2009) : IndependentClint DelacruzОценок пока нет
- NCP AneurysmДокумент4 страницыNCP AneurysmJanielle Christine Monsalud100% (1)
- NCP Chest PainДокумент2 страницыNCP Chest PainCG Patron BamboОценок пока нет
- NCP OsteoporosisДокумент5 страницNCP OsteoporosisAnonymous gAwcPNVRОценок пока нет
- Ncp'sДокумент8 страницNcp'sDuchess Kleine RafananОценок пока нет
- NCP Lack of KnowledgeДокумент3 страницыNCP Lack of KnowledgeFaye BartianaОценок пока нет
- Difflam Drug StudyДокумент1 страницаDifflam Drug StudyDanlee EstandaОценок пока нет
- Nursing Care PlanДокумент4 страницыNursing Care PlanSharmaine Grace Florig100% (2)
- Nursing Care Plan AДокумент6 страницNursing Care Plan ACrystal WyattОценок пока нет
- Self Care DeficitДокумент2 страницыSelf Care DeficitSj 斗力上75% (4)
- NCPДокумент4 страницыNCPEsther RefuncionОценок пока нет
- NCP SviДокумент4 страницыNCP SviEjie Boy IsagaОценок пока нет
- Post-Throidectomy Nursing Care PlanДокумент2 страницыPost-Throidectomy Nursing Care PlanCyrus De AsisОценок пока нет
- Compartment Syndrome NCP (PAIN)Документ2 страницыCompartment Syndrome NCP (PAIN)eunica16Оценок пока нет
- Self Care Deficit BahtingДокумент1 страницаSelf Care Deficit BahtingNaj SoliveresОценок пока нет
- NCP - Acute PainДокумент1 страницаNCP - Acute PainjsthrОценок пока нет
- Elderly NCPДокумент2 страницыElderly NCPGayzel Dela Cruz50% (2)
- Impaired Physical MobilityДокумент7 страницImpaired Physical MobilityVianah Eve EscobidoОценок пока нет
- NCP (BODY WEAKNESS)Документ3 страницыNCP (BODY WEAKNESS)Jum ChumОценок пока нет
- A Renal Failure (NCP)Документ2 страницыA Renal Failure (NCP)Julie Aranda Hapin100% (1)
- NCP AppendicitisДокумент1 страницаNCP AppendicitisNiña AngОценок пока нет
- Pre-Operative (Incision & Drainage of Abscess)Документ6 страницPre-Operative (Incision & Drainage of Abscess)Eunice MañalacОценок пока нет
- NCP Proper - Obstructive JaundiceДокумент8 страницNCP Proper - Obstructive JaundiceWyen Cabatbat100% (2)
- Nursing Care PlanДокумент13 страницNursing Care PlanCris Solis33% (3)
- Knowledge Deficit - RegorДокумент3 страницыKnowledge Deficit - RegorAdrian MallarОценок пока нет
- Care Plan ExampleДокумент2 страницыCare Plan Exampleincess27100% (1)
- HydroceleДокумент10 страницHydroceleRyan ReОценок пока нет
- NCP Deficient Fluid VolumeДокумент3 страницыNCP Deficient Fluid VolumeDoneva Lyn MedinaОценок пока нет
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationДокумент7 страницAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationpamelaideaОценок пока нет
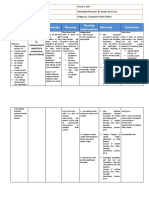
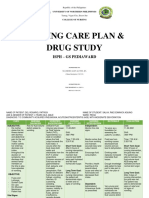
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Документ7 страницSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaОценок пока нет
- Feedings Down": Subjective Short Term Goal After DX Short Term GoalДокумент2 страницыFeedings Down": Subjective Short Term Goal After DX Short Term GoalTeddCamilingОценок пока нет
- HEALTH TEACHING PLAN For BREAST CANCERДокумент3 страницыHEALTH TEACHING PLAN For BREAST CANCERrod navales85% (13)
- Pathophysiology AHS HTN EДокумент1 страницаPathophysiology AHS HTN Erod navalesОценок пока нет
- HEALTH TEACHING PLAN For BREAST CANCERДокумент3 страницыHEALTH TEACHING PLAN For BREAST CANCERrod navales85% (13)
- HEALTH TEACHING PLAN For PCAPДокумент3 страницыHEALTH TEACHING PLAN For PCAProd navalesОценок пока нет
- ZENICAДокумент72 страницыZENICAVedadОценок пока нет
- Taller 8Документ2 страницыTaller 8monchito83hotmailesОценок пока нет
- Vital SignsДокумент3 страницыVital SignsNicole NipasОценок пока нет
- ADR Common Drug - Induced Organ DisordersДокумент45 страницADR Common Drug - Induced Organ Disorders0009439Оценок пока нет
- Cell Membranes and Transport TestДокумент3 страницыCell Membranes and Transport Testapi-252516966Оценок пока нет
- Anticholinergic DrugsДокумент19 страницAnticholinergic DrugseashshankarОценок пока нет
- Chapter 9 EndocrineДокумент40 страницChapter 9 EndocrineAiko EscobidoОценок пока нет
- Problem Set 2 EndocrinologyДокумент12 страницProblem Set 2 EndocrinologyJessica EtieneОценок пока нет
- Sodium Chloride Injection and Intravenous Infusion-PiДокумент4 страницыSodium Chloride Injection and Intravenous Infusion-PiNg Chee LunОценок пока нет
- What Is Ghrelin? Results Ghrelin Effecting Fat ScoresДокумент1 страницаWhat Is Ghrelin? Results Ghrelin Effecting Fat ScoresJihad Abou Ali WakedОценок пока нет
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyДокумент6 страницSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaОценок пока нет
- And Um-101Документ3 страницыAnd Um-101ver_at_workОценок пока нет
- Endocrine and Metabolic Disorders PDFДокумент31 страницаEndocrine and Metabolic Disorders PDFAna-Maria50% (2)
- Microbiota Therapy Acts via a Regulatory T Cell MyD88:RORγt Pathway to Suppress Food AllergyДокумент29 страницMicrobiota Therapy Acts via a Regulatory T Cell MyD88:RORγt Pathway to Suppress Food AllergyFelipe Gálvez JirónОценок пока нет
- Plant Growth Regulators (2014)Документ34 страницыPlant Growth Regulators (2014)matthewОценок пока нет
- Isometric Power Revolution Part2Документ86 страницIsometric Power Revolution Part2Smriti Ichopra100% (15)
- Urine Volatile Organic Compounds As Biomarkers For Minimal Change Type Nephrotic SyndromeДокумент24 страницыUrine Volatile Organic Compounds As Biomarkers For Minimal Change Type Nephrotic SyndromeYasser AlghrafyОценок пока нет
- Pathoma, Sketchy Pharm & Micro, B&B Video TimesДокумент52 страницыPathoma, Sketchy Pharm & Micro, B&B Video TimesAlina PolancoОценок пока нет
- Canine and Feline Endocrinology PDFДокумент685 страницCanine and Feline Endocrinology PDFSandra Solano100% (8)
- Weeks 3 - 8Документ32 страницыWeeks 3 - 8Stefan HutsonОценок пока нет
- Progr. PR., Simpozion Boli Genet Metab, Cluj-Napoca, 7-8 IunieДокумент3 страницыProgr. PR., Simpozion Boli Genet Metab, Cluj-Napoca, 7-8 IunieDoina Ababii UrsanОценок пока нет
- An Essential Role of The Mitochondrial Electron Transport Chain in Cell Proliferation Is To Enable Aspartate SynthesisДокумент13 страницAn Essential Role of The Mitochondrial Electron Transport Chain in Cell Proliferation Is To Enable Aspartate Synthesisyylf2016Оценок пока нет
- Shoku AnafilaktikДокумент16 страницShoku AnafilaktikindeenikeОценок пока нет
- Question PaperДокумент16 страницQuestion PaperAashi AkterОценок пока нет
- Utilidad Del Lactato Sérico Elevado Como Factor Pronóstico de Muerte en Sepsis SeveraДокумент6 страницUtilidad Del Lactato Sérico Elevado Como Factor Pronóstico de Muerte en Sepsis SeveraManuelito ZeОценок пока нет
- Anatomical Landmarks of Mandible: DR Hiba HamidДокумент29 страницAnatomical Landmarks of Mandible: DR Hiba HamidDr.Sathyabhama A.VОценок пока нет
- Summer Training For Speed: Alwyn Cosgrove's Training Design ProgramДокумент6 страницSummer Training For Speed: Alwyn Cosgrove's Training Design ProgramSteve HeywoodОценок пока нет
- Resp AssessmentДокумент19 страницResp AssessmentNURSES- NOOK & CORNERОценок пока нет
- SalbutamolДокумент5 страницSalbutamolFildehl Janice Bomediano CatipayОценок пока нет
- Emma Jordan - Research Final DraftДокумент7 страницEmma Jordan - Research Final Draftapi-436829682Оценок пока нет