Вам также может понравиться
- DehoffДокумент11 страницDehoffVictor Manuel Romero Herrera100% (4)
- Revision: Change Description Person Responsible, Name, Signature, Date Remark Revision Index CR NumberДокумент67 страницRevision: Change Description Person Responsible, Name, Signature, Date Remark Revision Index CR NumberAung Min Htet100% (1)
- Lumbar PunctureДокумент6 страницLumbar PunctureShesly Philomina100% (1)
- Bier Block (Intravenous Regional Anesthesia), Handout PDFДокумент8 страницBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamОценок пока нет
- Regional Anes 5Документ13 страницRegional Anes 5Shiva Kumar P SОценок пока нет
- Suctioning The TracheostomyДокумент16 страницSuctioning The TracheostomyJaily Mariano100% (1)
- Abdominal ParacentesisДокумент31 страницаAbdominal Paracentesisbala kumaaranОценок пока нет
- Procedure ON: EpisiotomyДокумент7 страницProcedure ON: EpisiotomyShalabh JoharyОценок пока нет
- Intravenous Fluid Insertion 2Документ56 страницIntravenous Fluid Insertion 2Genki Fay B. LequiganОценок пока нет
- NCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterДокумент7 страницNCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterIssaiah Nicolle CeciliaОценок пока нет
- CT4&5Документ10 страницCT4&5MARIA HILARY TABLANTEОценок пока нет
- Basic Ward ProceduresДокумент209 страницBasic Ward ProceduresNoopur SawarkarОценок пока нет
- Chest Tube InsertionДокумент4 страницыChest Tube InsertionElton Dias PinheiroОценок пока нет
- Ward Prep NotesДокумент7 страницWard Prep NotesReese Alessandra GandulfoОценок пока нет
- Thora Procedure 1Документ10 страницThora Procedure 1E PadzОценок пока нет
- Nasotracheal SuctioningДокумент2 страницыNasotracheal Suctioningmarie100% (3)
- Caudal Epidural InjectionДокумент6 страницCaudal Epidural InjectionRS BaptisОценок пока нет
- Government College of Nursing: Procedure ONДокумент6 страницGovernment College of Nursing: Procedure ONpriyanka100% (6)
- Thoracentesis - ClinicalKey (1) (11-23)Документ13 страницThoracentesis - ClinicalKey (1) (11-23)jose luisОценок пока нет
- Abdominalparacentesis 131005010712 Phpapp02Документ33 страницыAbdominalparacentesis 131005010712 Phpapp02Shrish Pratap SinghОценок пока нет
- Or Write Up (Appendectomy) : Pines City Colleges College of NursingДокумент9 страницOr Write Up (Appendectomy) : Pines City Colleges College of Nursingthomasfinley44Оценок пока нет
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Документ13 страницSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanОценок пока нет
- SOPs To Deliver Safe Paediatric CareДокумент11 страницSOPs To Deliver Safe Paediatric Carearadhya asthanaОценок пока нет
- Nur 146 RleДокумент47 страницNur 146 RleKeziah Marie Chua Santa-AnaОценок пока нет
- 9, Procedure of PICCДокумент9 страниц9, Procedure of PICCputriseptinaОценок пока нет
- Craven & Hirnle's Nursing Procedures and Fundamentals OnlineДокумент4 страницыCraven & Hirnle's Nursing Procedures and Fundamentals Onlineisapatrick8126Оценок пока нет
- Central Venous CatheterДокумент5 страницCentral Venous Catheterrajnishpathak648Оценок пока нет
- Suctioning The Nasopharygeal and Oropharyngeal AirwaysДокумент8 страницSuctioning The Nasopharygeal and Oropharyngeal AirwaysChamelli RobinОценок пока нет
- Ghising Astak Episiotomy and RepairДокумент3 страницыGhising Astak Episiotomy and Repairastak ghisingОценок пока нет
- Final 16-17Документ5 страницFinal 16-17Churrizo IslamiОценок пока нет
- Intravenous Regonal Anaesthesia Biers BlockДокумент2 страницыIntravenous Regonal Anaesthesia Biers BlockOkenabirhieОценок пока нет
- Removing A Nasogastric Tube22Документ4 страницыRemoving A Nasogastric Tube22Ashraf QotmoshОценок пока нет
- CVP MonitoringДокумент10 страницCVP MonitoringRaghu RajanОценок пока нет
- Knee Joint AND Hip Joint PuncturesДокумент13 страницKnee Joint AND Hip Joint PuncturesTimbur IgorОценок пока нет
- Retdem (Ivt & BT)Документ11 страницRetdem (Ivt & BT)Wonie booОценок пока нет
- ALS-Adult All ProtocolsДокумент54 страницыALS-Adult All ProtocolsNur SusiawantyОценок пока нет
- Epidural AnesthesiaДокумент32 страницыEpidural AnesthesiaAmareОценок пока нет
- Rapid Sequence Intubation: BY Budak KecikДокумент25 страницRapid Sequence Intubation: BY Budak KecikAqua ForceОценок пока нет
- Assisting Iv InfusionДокумент3 страницыAssisting Iv InfusionDianne LabisОценок пока нет
- Tgs Chelsa Individu Mr. BingsДокумент4 страницыTgs Chelsa Individu Mr. Bingsjeffriwahyudi91Оценок пока нет
- Procedure On Lumber PunctureДокумент8 страницProcedure On Lumber PunctureDimpal ChoudharyОценок пока нет
- Ovariectomy Via Colpotomy ApproachДокумент5 страницOvariectomy Via Colpotomy ApproachMeredithWindhorseHudes-Lowder100% (1)
- Sub Arachnoid BlockДокумент32 страницыSub Arachnoid Blockhendra_darmawan_4Оценок пока нет
- Final Osce?Документ5 страницFinal Osce?Queen ShОценок пока нет
- Spinal AnesthesiaДокумент7 страницSpinal AnesthesiaAlaa OmarОценок пока нет
- Procedures ThoracentesisДокумент4 страницыProcedures ThoracentesisPatty MArivel ReinosoОценок пока нет
- Minor Surgical Procedures...Документ10 страницMinor Surgical Procedures...Silinna May Lee SanicoОценок пока нет
- Nursing Care Management 109: de La Salle Lipa College of NursingДокумент3 страницыNursing Care Management 109: de La Salle Lipa College of NursingZyra DIOKNOОценок пока нет
- Lynn15 1Документ4 страницыLynn15 1Harley Justiniani Dela CruzОценок пока нет
- Pneumothorax GuidelineДокумент8 страницPneumothorax GuidelineIonut - Eugen IonitaОценок пока нет
- Suturing Perineal Lacerations EditedДокумент5 страницSuturing Perineal Lacerations EditedJanzell Anne Borja AlbaniaОценок пока нет
- Removing A Nasogastric TubeДокумент4 страницыRemoving A Nasogastric TubeAshraf QotmoshОценок пока нет
- Spinal AnasethesiaДокумент5 страницSpinal AnasethesiaHiBå ÂwÅð ĀŁ-ťømОценок пока нет
- Guidelines To The Nurse's Role in The ManagementДокумент16 страницGuidelines To The Nurse's Role in The ManagementKezia ImanuellaОценок пока нет
- Open Cholecystectomy DictationДокумент4 страницыOpen Cholecystectomy DictationHassanОценок пока нет
- Pipelle Endometrial Suction Curette Instructions For Use PDFДокумент20 страницPipelle Endometrial Suction Curette Instructions For Use PDFBernadette YapОценок пока нет
- SOP: Retro-Orbital Blood Collection in The RatДокумент5 страницSOP: Retro-Orbital Blood Collection in The RatSipend AnatomiОценок пока нет
- OB2 RLE SAS 6 Versions SAS 7 Caesarian Section SAS 8 Uterine AtonyДокумент26 страницOB2 RLE SAS 6 Versions SAS 7 Caesarian Section SAS 8 Uterine AtonyHana LandinginОценок пока нет
- Assisting in Intravenous Infusion NewДокумент52 страницыAssisting in Intravenous Infusion NewDianne LabisОценок пока нет
- No Author's Name Name For Citation Title Journal Name Year NoДокумент5 страницNo Author's Name Name For Citation Title Journal Name Year NovennaОценок пока нет
- Bismillah Daftar Pustaka IbdДокумент3 страницыBismillah Daftar Pustaka IbdvennaОценок пока нет
- Daftar Pustaka PROLAPSUS UTERIДокумент3 страницыDaftar Pustaka PROLAPSUS UTERIvennaОценок пока нет
- Urinary Incontinence Jam A 2017Документ13 страницUrinary Incontinence Jam A 2017vennaОценок пока нет
- Lab Exe No. 10 - Design of Simple Bioethanol Production System - FermentationДокумент2 страницыLab Exe No. 10 - Design of Simple Bioethanol Production System - FermentationJamil Mansor M. LaguiabОценок пока нет
- Theoretical Analysis of Production of Di-Nitro Stilbene Di-Sulphonic Acid (DASDAДокумент68 страницTheoretical Analysis of Production of Di-Nitro Stilbene Di-Sulphonic Acid (DASDAvenky100% (1)
- 14 - Part 3 - Ch. 7 - A Lesson With Czerny - Tempo Rubato PDFДокумент21 страница14 - Part 3 - Ch. 7 - A Lesson With Czerny - Tempo Rubato PDFErduandОценок пока нет
- Sef 0l6aeДокумент144 страницыSef 0l6aezarni zarniОценок пока нет
- Dos Vs Linux CommandsДокумент23 страницыDos Vs Linux CommandsSomasekhar Chowdary KakaralaОценок пока нет
- Salem Etal TLE 2007Документ5 страницSalem Etal TLE 2007BILLY CHAVEZ CHAMPIОценок пока нет
- (Methods in Molecular Medicine) S. Moira Brown, Alasdair R. MacLean - Herpes Simplex Virus Protocols (1998, Humana Press)Документ406 страниц(Methods in Molecular Medicine) S. Moira Brown, Alasdair R. MacLean - Herpes Simplex Virus Protocols (1998, Humana Press)Rares TautОценок пока нет
- Topic 9 - The Standard Capital Asset Pricing Model Question PDFДокумент15 страницTopic 9 - The Standard Capital Asset Pricing Model Question PDFSrinivasa Reddy SОценок пока нет
- Petrel 2013 Property Modeling Course: Module 2: Data PreparationДокумент15 страницPetrel 2013 Property Modeling Course: Module 2: Data PreparationJaninne Campo100% (1)
- Deepwater Development OverviewДокумент11 страницDeepwater Development OverviewBarry HiiОценок пока нет
- Manuel Guindeau X2Документ53 страницыManuel Guindeau X2fr_emailleОценок пока нет
- Voltaje en El EjeДокумент48 страницVoltaje en El EjeRigoberto UrrutiaОценок пока нет
- Service Bulletin RT-18.4: Technical Information To All Owners / Operators of Wärtsilä RTA and RT-flex EnginesДокумент14 страницService Bulletin RT-18.4: Technical Information To All Owners / Operators of Wärtsilä RTA and RT-flex Engineszbkt07Оценок пока нет
- ISEB CE CASE Mathematics 13 Specification 2020 11.22Документ35 страницISEB CE CASE Mathematics 13 Specification 2020 11.22agastyazadОценок пока нет
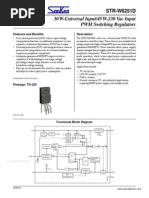
- Datasheet PDFДокумент15 страницDatasheet PDFperro sОценок пока нет
- Navistar Diagnostic Trouble Codes EGES395 - DTCДокумент8 страницNavistar Diagnostic Trouble Codes EGES395 - DTCjpablop1278% (9)
- Mud Logging Technical Document PDFДокумент153 страницыMud Logging Technical Document PDFasjad raja100% (5)
- Conduction Convection RadiationДокумент23 страницыConduction Convection Radiationsuhaila bakarОценок пока нет
- 22-01 Simple Linear Motion 1Документ1 страница22-01 Simple Linear Motion 1David BumbaloughОценок пока нет
- DRIVEN PilesДокумент64 страницыDRIVEN PilesAyoОценок пока нет
- Botta-Dukát 2005 (RaoQ)Документ8 страницBotta-Dukát 2005 (RaoQ)BeatrizОценок пока нет
- UGRD-ECE6205-Signals-Spectra-and-Signal-Processing-legit-not-quizess MidALLДокумент19 страницUGRD-ECE6205-Signals-Spectra-and-Signal-Processing-legit-not-quizess MidALLJitlee Papa100% (3)
- Cre 2Документ42 страницыCre 2Sagar ChandegaraОценок пока нет
- Super Had CCD IIДокумент2 страницыSuper Had CCD IIMohd Safian ZakariaОценок пока нет
- Cross Reference Odpowiedniki - DanfossДокумент29 страницCross Reference Odpowiedniki - DanfossDanielEscobarMontecinosОценок пока нет
- Galleon NTS-6002-GPS DatasheetДокумент3 страницыGalleon NTS-6002-GPS DatasheetObdulio SantanaОценок пока нет
- Irf2807 International DatasheetДокумент8 страницIrf2807 International DatasheetAdam SchwemleinОценок пока нет
- Software Development Life Cycle-VДокумент3 страницыSoftware Development Life Cycle-VDeepak Prakash JayaОценок пока нет