Вам также может понравиться
- Age With Moderate Dehydration New 1Документ74 страницыAge With Moderate Dehydration New 1Jhade Relleta100% (1)
- Acute Gastro Enteritis Case StudyДокумент71 страницаAcute Gastro Enteritis Case Studygiadda100% (2)
- Anatomy and Physiology of Acute GastroenteritisДокумент4 страницыAnatomy and Physiology of Acute GastroenteritisAnne Lorraine Rodriguez91% (11)
- Case Presentation (Age) NG Grp. A2 FinalДокумент43 страницыCase Presentation (Age) NG Grp. A2 Finaljean therese83% (6)
- Acute Gastroenteritis Case StudyДокумент20 страницAcute Gastroenteritis Case StudyJohn Carlo Kimura Rabanes100% (1)
- Acute Gastroenteritis (Meta)Документ77 страницAcute Gastroenteritis (Meta)Al-nazer Azer AlОценок пока нет
- AGE PathophysiologyДокумент2 страницыAGE Pathophysiologyjosephcanlas67% (3)
- Acute Gastroenteristis Case Study GRP 3Документ22 страницыAcute Gastroenteristis Case Study GRP 3juel_navarro86% (7)
- Pathophysiology of Acute GastroenteritisДокумент1 страницаPathophysiology of Acute GastroenteritisAiza Yee Bacani83% (6)
- CASE STUDY of AGE With Moderate DehydrationДокумент24 страницыCASE STUDY of AGE With Moderate DehydrationHikaru Takishima100% (2)
- Acute GastroenteritisДокумент19 страницAcute GastroenteritisJoy Jarin100% (1)
- Case Study AGE With DehydrationДокумент12 страницCase Study AGE With Dehydrationmwdlc_22100% (2)
- Acute GastroenteritisДокумент31 страницаAcute GastroenteritismariasomorayОценок пока нет
- Case Study AGE With Signs of DehydrationДокумент27 страницCase Study AGE With Signs of Dehydrationtansincos100% (23)
- NCP GastroenteritisДокумент1 страницаNCP GastroenteritisFranchesca PaunganОценок пока нет
- Pathophysiology of Acute GastroenteritisДокумент1 страницаPathophysiology of Acute GastroenteritisAlliah Grejie AnneОценок пока нет
- Pa Tho Physiology of Acute GastroenteritisДокумент2 страницыPa Tho Physiology of Acute Gastroenteritisromeo rivera100% (16)
- Nursing Case Study Acute GastroДокумент8 страницNursing Case Study Acute GastroEdilyn BalicaoОценок пока нет
- Case Presentation: Acute GastroenteritisДокумент60 страницCase Presentation: Acute GastroenteritisBeverly Datu80% (5)
- PathophysiologyДокумент3 страницыPathophysiologyKita kita100% (1)
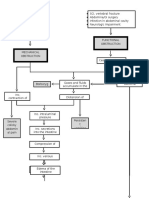
- Pathophysiology of Intestinal ObstructionДокумент2 страницыPathophysiology of Intestinal ObstructionMatthew Rich Laguitao CortesОценок пока нет
- Case For Acute GastroenteritisДокумент26 страницCase For Acute GastroenteritisSheana TmplОценок пока нет
- Pathophy (Age)Документ1 страницаPathophy (Age)Michelle Ann CasamayorОценок пока нет
- Drug StudyДокумент4 страницыDrug StudyZyra SantosОценок пока нет
- Acute GastroenteritisДокумент56 страницAcute Gastroenteritisneil052298% (46)
- TITLE: Prevention of Diarrhea: A Health Teaching PlanДокумент3 страницыTITLE: Prevention of Diarrhea: A Health Teaching PlanMariel Gamalo0% (1)
- CS5 (AGE) Acute Gastroenteritis NCPДокумент2 страницыCS5 (AGE) Acute Gastroenteritis NCPAudrie Allyson GabalesОценок пока нет
- Acute Gastroenteritis With Moderate DehydrationДокумент28 страницAcute Gastroenteritis With Moderate DehydrationSan Dee71% (7)
- Discharge Plan GastroenteritisДокумент2 страницыDischarge Plan Gastroenteritisneil0522100% (14)
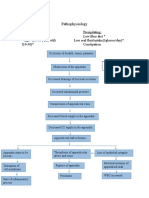
- Appendicitis PathophysiologyДокумент2 страницыAppendicitis PathophysiologyitsmeayaОценок пока нет
- Acute Gastroenteritis Case StudyДокумент19 страницAcute Gastroenteritis Case Studykirstenpapera100% (54)
- Pathophysiology of Acute GastroenteritisДокумент5 страницPathophysiology of Acute Gastroenteritisheron_bayanin_15Оценок пока нет
- Case Study On AGEДокумент28 страницCase Study On AGEzyxert100% (19)
- Gastroenteritis Care StudyДокумент13 страницGastroenteritis Care StudyÄxxö Ahkö Hinoguin50% (2)
- Acute GastroenteritisДокумент29 страницAcute GastroenteritisMASII100% (13)
- Acute Gastroenteritis Powerpoint #1Документ122 страницыAcute Gastroenteritis Powerpoint #1Marlone C. Nadunza78% (9)
- Pathophysiology Acute Gastroenteritis AGEДокумент3 страницыPathophysiology Acute Gastroenteritis AGEVHyneh Basher80% (5)
- Individual Case Study Acute GlomerulonephritisДокумент26 страницIndividual Case Study Acute GlomerulonephritisBatrisyia HalimsОценок пока нет
- Salmonella, Campylobacter, Yersinia Enterocolitica and Shigella InfectionsДокумент3 страницыSalmonella, Campylobacter, Yersinia Enterocolitica and Shigella InfectionsKelvin BolusanОценок пока нет
- Gastroenteritis in Adults and Older Children: EpidemiologyДокумент4 страницыGastroenteritis in Adults and Older Children: Epidemiologyjotq19Оценок пока нет
- Gastrointestinal Tract Diarrhea Nausea Viral Infection BacteriaДокумент60 страницGastrointestinal Tract Diarrhea Nausea Viral Infection BacteriawakuyllibОценок пока нет
- GastroenteritisДокумент3 страницыGastroenteritisNicoleОценок пока нет
- Case Presentation GastroenteritisДокумент58 страницCase Presentation GastroenteritisShereen Manabilang100% (3)
- Patofisiologi DiareДокумент45 страницPatofisiologi DiareAngela Kristiana Intan100% (1)
- Diarrhea - StatPearls - NCBI BookshelfДокумент4 страницыDiarrhea - StatPearls - NCBI BookshelfIndira SellyОценок пока нет
- Gastroenteritis CausesДокумент6 страницGastroenteritis CausesMikael AlmstrongОценок пока нет
- GastroenteritisДокумент2 страницыGastroenteritisIanne MerhОценок пока нет
- Acute GastroenteritisДокумент7 страницAcute GastroenteritisCherr NollОценок пока нет
- Diarrhea: Cause Signs and Symptoms Pathophysiolog Y Prognosis StatisticsДокумент13 страницDiarrhea: Cause Signs and Symptoms Pathophysiolog Y Prognosis StatisticsRogie SaludoОценок пока нет
- Gastroenteritis Gastrointestinal Tract: Clostridium DifficileДокумент14 страницGastroenteritis Gastrointestinal Tract: Clostridium DifficilemichunmeeadОценок пока нет
- There Are Two Main Types of GastritisДокумент11 страницThere Are Two Main Types of GastritisMike Faustino SolangonОценок пока нет
- When "Warteg" Gives Him More: Group 7Документ46 страницWhen "Warteg" Gives Him More: Group 7Daniel Hans JayaОценок пока нет
- Diarrhea: Practice Essentials, Background, PathophysiologyДокумент6 страницDiarrhea: Practice Essentials, Background, PathophysiologyBilal El BariОценок пока нет
- Acute GastroenteritisДокумент35 страницAcute GastroenteritisAdil ShabbirОценок пока нет
- Acute Gastroenteritis: Acute Inflammation of The Stomach Small IntestineДокумент6 страницAcute Gastroenteritis: Acute Inflammation of The Stomach Small IntestineJha FernandoОценок пока нет
- Anatomy and Physiology of The Digestive SystemДокумент5 страницAnatomy and Physiology of The Digestive SystemKate Cris TalatagodОценок пока нет
- A Simple Guide to Gastritis and Related ConditionsОт EverandA Simple Guide to Gastritis and Related ConditionsРейтинг: 4.5 из 5 звезд4.5/5 (3)
- Secretory Diarrhea Causes: CholeraДокумент8 страницSecretory Diarrhea Causes: CholerasakuraleeshaoranОценок пока нет
- Common Pediatric IllnessesДокумент9 страницCommon Pediatric IllnessesZeraОценок пока нет
- Elimination DisordersДокумент111 страницElimination DisordersKarina Blanca Sanico AdranedaОценок пока нет
- CA Breast New ChangedДокумент72 страницыCA Breast New Changedbenak shivalingappaОценок пока нет
- Uro Spots SummaryДокумент25 страницUro Spots Summarynthabiseng maboganaОценок пока нет
- Hyperkalemia: Dr. K. K. Gupta Associate Prof. Department of Medicine, KgmuДокумент23 страницыHyperkalemia: Dr. K. K. Gupta Associate Prof. Department of Medicine, KgmuPrass Ekasetia PoetraОценок пока нет
- Acid/Base and ABG Interpretation Made SimpleДокумент45 страницAcid/Base and ABG Interpretation Made SimpleekadtorОценок пока нет
- Prostate 4.2.0.0.rel CapcpДокумент26 страницProstate 4.2.0.0.rel CapcpkarimahihdaОценок пока нет
- Paper AnalysisДокумент4 страницыPaper AnalysisLayali MassisОценок пока нет
- Predicting End of Life: de Anna Looper, RN CHPNДокумент4 страницыPredicting End of Life: de Anna Looper, RN CHPNSathiswebОценок пока нет
- Syncope & PalpitationДокумент2 страницыSyncope & PalpitationArjunОценок пока нет
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicДокумент19 страницLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroОценок пока нет
- Selected Anomalies and Diseases of The Eye: Compiled by Virginia E. Bishop, Ph.D. 1986Документ57 страницSelected Anomalies and Diseases of The Eye: Compiled by Virginia E. Bishop, Ph.D. 1986Matthew MckenzieОценок пока нет
- ANC and BFДокумент29 страницANC and BFRose Anne Tusi BotinОценок пока нет
- Nicotine: How Does Nicotine Deliver Its Effect?Документ6 страницNicotine: How Does Nicotine Deliver Its Effect?jmolaecheaОценок пока нет
- Pop Jordanova 67 76Документ10 страницPop Jordanova 67 76lakimkОценок пока нет
- SAJD Vol 7 No 4 November 2014Документ41 страницаSAJD Vol 7 No 4 November 2014Anupam BhardwajОценок пока нет
- Pancreatic PseudocystДокумент16 страницPancreatic PseudocystSpandan KadamОценок пока нет
- Widya Kusumaningrum (1902114) 2C Tugas Bhs. Inggris Asking The Dimensions of SymptomДокумент4 страницыWidya Kusumaningrum (1902114) 2C Tugas Bhs. Inggris Asking The Dimensions of SymptomWidya KusumaningrumОценок пока нет
- Arachnoid CystДокумент4 страницыArachnoid CystSlaviša KovačevićОценок пока нет
- Managing The Red Eye: Speaker NotesДокумент46 страницManaging The Red Eye: Speaker NotesAlina DănescuОценок пока нет
- Fast Chicken Pox Cure PDF-eBook, Stefan HallДокумент46 страницFast Chicken Pox Cure PDF-eBook, Stefan HallCyrusОценок пока нет
- Ramos-2bn NCP Delivery RoomДокумент2 страницыRamos-2bn NCP Delivery RoomLouwella RamosОценок пока нет
- 404 Veterinary Referral Hospital - BrochureДокумент11 страниц404 Veterinary Referral Hospital - BrochureJoanne FagnouОценок пока нет
- Ma. Theresa O. Bermudez 4BSN1/ GroupДокумент4 страницыMa. Theresa O. Bermudez 4BSN1/ GroupJenna AbuanОценок пока нет
- Lewy Body DementiaДокумент20 страницLewy Body DementiaAbdul SadiqОценок пока нет
- Essay - Child DevelopmentДокумент2 страницыEssay - Child DevelopmentTina AroraОценок пока нет
- Definition:: Pleural EffusionДокумент4 страницыDefinition:: Pleural EffusionGetom NgukirОценок пока нет
- 16 Corneal DegenerationsДокумент11 страниц16 Corneal DegenerationsIrma FloresОценок пока нет
- Strataderm BrochureДокумент2 страницыStrataderm BrochureBakateriaОценок пока нет
- Dental Risk Assessment FormДокумент2 страницыDental Risk Assessment FormSamantha TacadОценок пока нет
- Luaran Perdarahan Intraventrikel Yang Dilakukan Operasi Di Departemen Bedah Saraf Rsupn Dr. Cipto MangunkusumoДокумент5 страницLuaran Perdarahan Intraventrikel Yang Dilakukan Operasi Di Departemen Bedah Saraf Rsupn Dr. Cipto MangunkusumoMerry AndrianyОценок пока нет
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Документ3 страницыStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYОценок пока нет