Вам также может понравиться
- Flowchart 1 Immediate Management of An AsphyxiatednewbornДокумент3 страницыFlowchart 1 Immediate Management of An Asphyxiatednewborndessy pratiwiОценок пока нет
- Flowchart 1 Immediate Management of An Asphyxiated NewbornДокумент3 страницыFlowchart 1 Immediate Management of An Asphyxiated Newborndessy pratiwiОценок пока нет
- Shock PresentationДокумент20 страницShock Presentationrosalyn sugayОценок пока нет
- Shock PresentationДокумент20 страницShock PresentationvgmanjunathОценок пока нет
- MIS C Algorithim Version 2Документ8 страницMIS C Algorithim Version 2Saima UmairОценок пока нет
- Paediatric Septic ShockДокумент37 страницPaediatric Septic ShockJavedgouri GouriОценок пока нет
- Severe Sepsisand Septic Shock GuidelinesДокумент17 страницSevere Sepsisand Septic Shock GuidelinesdrquamrulОценок пока нет
- On Call ComplaintsДокумент3 страницыOn Call ComplaintsrashaОценок пока нет
- Paediatric Septic ShockДокумент34 страницыPaediatric Septic ShockSudha YadavОценок пока нет
- 322 Convulsions and Status EpilepticusДокумент7 страниц322 Convulsions and Status EpilepticusMohammad Irfan khanОценок пока нет
- Total Body HypothermiaДокумент5 страницTotal Body HypothermiaDwi Jaya MadeОценок пока нет
- Circulation July 2020Документ25 страницCirculation July 2020Siva RamanОценок пока нет
- Febrile Seizures: Status EpilepticusДокумент34 страницыFebrile Seizures: Status EpilepticusSAIMA BATOOLОценок пока нет
- Hypoxic Ischaemic Encephalopathy HIE AsphyxiaДокумент6 страницHypoxic Ischaemic Encephalopathy HIE AsphyxiaCaity YoungОценок пока нет
- Recent Advances in The Treatment of ShockДокумент52 страницыRecent Advances in The Treatment of ShockasupicuОценок пока нет
- Cme: Dengue Fever: by Nur ShafikaДокумент47 страницCme: Dengue Fever: by Nur ShafikaSyuk IdhamОценок пока нет
- Neonatal SeizuresДокумент4 страницыNeonatal SeizuresHaitham HafezОценок пока нет
- K4 - Asfiksia NeonatorumДокумент35 страницK4 - Asfiksia NeonatorumNatasya VianaОценок пока нет
- Neonatal AsphyxiaДокумент35 страницNeonatal AsphyxiaAsha jilu67% (3)
- Evaluation and Management of Status Epilepticus in ChildrenДокумент13 страницEvaluation and Management of Status Epilepticus in ChildrenAyan BiswasОценок пока нет
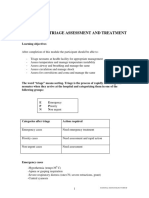
- Emergency Triage Assessment and Treatment: National Neonatology ForumДокумент6 страницEmergency Triage Assessment and Treatment: National Neonatology ForumSatya Prakash TiwariОценок пока нет
- CD CompleteДокумент19 страницCD CompletebhibhiОценок пока нет
- Emergency Drugs (LEAD)Документ8 страницEmergency Drugs (LEAD)RayePrudenteОценок пока нет
- RSVДокумент15 страницRSVbtheresakОценок пока нет
- Night Float VAДокумент9 страницNight Float VAkirОценок пока нет
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungДокумент47 страницKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiОценок пока нет
- CH 073 Shock in Office PracticeДокумент8 страницCH 073 Shock in Office PracticeLaxmikant RathiОценок пока нет
- An Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNДокумент49 страницAn Introduction To Obstetrical Emergencies: Charles D Giordano CRNA, MSNEffendi ZakriОценок пока нет
- Status Elipticus April 2018Документ2 страницыStatus Elipticus April 2018walidОценок пока нет
- Guideline For Management Protocol of Children With Fever and Respiratory SymptomsДокумент44 страницыGuideline For Management Protocol of Children With Fever and Respiratory SymptomsKushagr GautamОценок пока нет
- Management of Shock in ChildrenДокумент26 страницManagement of Shock in ChildrenkarinakerenОценок пока нет
- Pediatric Protokol EmergencyДокумент19 страницPediatric Protokol EmergencyChristian RobbyОценок пока нет
- Resusitasi CairanДокумент48 страницResusitasi Cairanadi tiarmanОценок пока нет
- ConnectorДокумент4 страницыConnectoryetaung8Оценок пока нет
- Syock & ManagementДокумент34 страницыSyock & ManagementIndra Anwari RukmanОценок пока нет
- Pediatric Emergencies: Presented By: Ziyad SalihДокумент51 страницаPediatric Emergencies: Presented By: Ziyad SalihNana MuktiОценок пока нет
- 1538 Exam 5 IntracranialДокумент31 страница1538 Exam 5 IntracranialJade EdanoОценок пока нет
- Case StudyДокумент46 страницCase StudysarikaОценок пока нет
- Hayats ResponsesДокумент18 страницHayats Responsesyacineone01Оценок пока нет
- FUNDAДокумент17 страницFUNDAMarcel TabucolОценок пока нет
- Management Protocol of Septic Shock: DiagnosisДокумент3 страницыManagement Protocol of Septic Shock: Diagnosissky nutsОценок пока нет
- FaciitisДокумент17 страницFaciitisdalaginding clophОценок пока нет
- Clinical Management JEДокумент15 страницClinical Management JEegalivanОценок пока нет
- Care of The Newborn: By: Myra DG. Angeles, RN, MANДокумент44 страницыCare of The Newborn: By: Myra DG. Angeles, RN, MANMyra De Guzman AngelesОценок пока нет
- Shock SummaryДокумент1 страницаShock SummaryTeoh KWОценок пока нет
- JMD PPH Critical Thinking Map-1Документ1 страницаJMD PPH Critical Thinking Map-1api-417952873Оценок пока нет
- Randolph Cornelio M. Capon, BSN, RNДокумент42 страницыRandolph Cornelio M. Capon, BSN, RNhassen zabalaОценок пока нет
- 7698alorithm SeizureДокумент3 страницы7698alorithm Seizureboromeus abyasa daniswara100% (1)
- Pediatric Mock Resuscitation ScenariosДокумент6 страницPediatric Mock Resuscitation ScenariosdinkytinkОценок пока нет
- Syncope: - Selvarathi KДокумент27 страницSyncope: - Selvarathi KSelvarathi KandhaswamyОценок пока нет
- Paediatrics The Unconscious Child: GCS Measurement in ChildrenДокумент2 страницыPaediatrics The Unconscious Child: GCS Measurement in Childrenrekha meenaОценок пока нет
- Ob2 Sas 34Документ6 страницOb2 Sas 34????Оценок пока нет
- Medicine Test On CVS Respiratory EndocrinologyДокумент10 страницMedicine Test On CVS Respiratory EndocrinologyNavid BabluОценок пока нет
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmДокумент11 страницHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuОценок пока нет
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Документ9 страницO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasОценок пока нет
- Neonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikДокумент21 страницаNeonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikbidisОценок пока нет
- OB - Hypertensive DisordersДокумент4 страницыOB - Hypertensive DisordersJasmine Nicole RemetreОценок пока нет
- Intubations Outside ICUДокумент79 страницIntubations Outside ICUzulham effendyОценок пока нет
- Neonatal ShockДокумент50 страницNeonatal ShockBenazir Nabilla RojwaaОценок пока нет
- NCLEX Educational Program Codes PDFДокумент110 страницNCLEX Educational Program Codes PDFKim MedairosОценок пока нет
- NCLEX Educational Program Codes PDFДокумент110 страницNCLEX Educational Program Codes PDFKim MedairosОценок пока нет
- The Pearls For NCLEX Review in Publisher March PDFДокумент34 страницыThe Pearls For NCLEX Review in Publisher March PDFKim Medairos100% (3)
- Nclex RN Reg Questions Amp Answers Made Incredibly Easy 2891831Документ4 страницыNclex RN Reg Questions Amp Answers Made Incredibly Easy 2891831Kim Medairos100% (1)
- NCLEX Seminar ManuscriptДокумент53 страницыNCLEX Seminar ManuscriptKim Medairos100% (1)
- IELTS Free Practice Test Answer SheetДокумент6 страницIELTS Free Practice Test Answer SheetKim MedairosОценок пока нет
- IELTS Free Practice TestДокумент22 страницыIELTS Free Practice TestKim MedairosОценок пока нет
- IELTS Free Practice TestДокумент22 страницыIELTS Free Practice TestKim MedairosОценок пока нет
- South San Francisco Talks Plans For Sports Park ImprovementsДокумент32 страницыSouth San Francisco Talks Plans For Sports Park ImprovementsSan Mateo Daily JournalОценок пока нет
- Turning The Mind Into An AllyДокумент244 страницыTurning The Mind Into An AllyNic Sosa67% (3)
- Assignment On Unstable or Astatic Gravimeters and Marine Gravity SurveyДокумент9 страницAssignment On Unstable or Astatic Gravimeters and Marine Gravity Surveyraian islam100% (1)
- Cyanocobalamin Injection Clinical Pharmacology Drug MonographДокумент36 страницCyanocobalamin Injection Clinical Pharmacology Drug MonographLaureyОценок пока нет
- Finite Element Modeling Analysis of Nano Composite Airfoil StructureДокумент11 страницFinite Element Modeling Analysis of Nano Composite Airfoil StructureSuraj GautamОценок пока нет
- LEARNING ACTIVITY SHEET in Oral CommДокумент4 страницыLEARNING ACTIVITY SHEET in Oral CommTinTin100% (1)
- Language Loss in Waray: Ni Voltaire Q. UyzonДокумент23 страницыLanguage Loss in Waray: Ni Voltaire Q. UyzonMary Rose OmbrogОценок пока нет
- PS410Документ2 страницыPS410Kelly AnggoroОценок пока нет
- Directorate of Technical Education, Maharashtra StateДокумент47 страницDirectorate of Technical Education, Maharashtra StatePandurang GunjalОценок пока нет
- Diagnostic Test - Tle8Документ2 страницыDiagnostic Test - Tle8rose mae marambaОценок пока нет
- Challenges Affecting Devolution PDFДокумент94 страницыChallenges Affecting Devolution PDFELIJAH M. OMBEOОценок пока нет
- Case Study 1 HRM in PandemicДокумент2 страницыCase Study 1 HRM in PandemicKristine Dana LabaguisОценок пока нет
- The Big M Method: Group BДокумент7 страницThe Big M Method: Group BWoo Jin YoungОценок пока нет
- This Study Resource Was: MCV4U Exam ReviewДокумент9 страницThis Study Resource Was: MCV4U Exam ReviewNathan WaltonОценок пока нет
- Adel Lock ManualДокумент1 страницаAdel Lock Manual24245677843Оценок пока нет
- STORIESДокумент18 страницSTORIESHaRa TОценок пока нет
- Philips fwt9200Документ37 страницPhilips fwt9200Alex BrazОценок пока нет
- Jungbluth Main Catalogue-LanacДокумент60 страницJungbluth Main Catalogue-LanacMilenkoBogdanovicОценок пока нет
- Answer KeyДокумент4 страницыAnswer KeyLouina YnciertoОценок пока нет
- Application Tracking System: Mentor - Yamini Ma'AmДокумент10 страницApplication Tracking System: Mentor - Yamini Ma'AmBHuwanОценок пока нет
- Cascade Configuration Tool: Installation and Operations ManualДокумент22 страницыCascade Configuration Tool: Installation and Operations ManualAndrés GarciaОценок пока нет
- IRAQ Reproductive Maternal, Newborn, Child and Adolescent HealthДокумент32 страницыIRAQ Reproductive Maternal, Newborn, Child and Adolescent HealthbejarhasanОценок пока нет
- Root End Filling MaterialsДокумент9 страницRoot End Filling MaterialsRuchi ShahОценок пока нет
- Accenture MockДокумент1 страницаAccenture Mockrajyogesh487Оценок пока нет
- Ias Book 2015Документ49 страницIas Book 2015Rahul SharmaОценок пока нет
- Data Abstraction and Problem Solving With C Walls and Mirrors 6th Edition Carrano Solutions ManualДокумент36 страницData Abstraction and Problem Solving With C Walls and Mirrors 6th Edition Carrano Solutions Manualallocaturnonylgvtt100% (12)
- Ageing World ReportДокумент4 страницыAgeing World Reporttheresia anggitaОценок пока нет
- Bach Polonaise G Min BWV 119 A4Документ1 страницаBach Polonaise G Min BWV 119 A4vincenzovaiaОценок пока нет
- 14 Days of Prayer and FastingДокумент40 страниц14 Days of Prayer and FastingntsakoramphagoОценок пока нет
- Chapter 34 Esip For FinalДокумент35 страницChapter 34 Esip For FinalJeaniel BorlingОценок пока нет