Вам также может понравиться
- Vital Judo Throwing TechniquesДокумент193 страницыVital Judo Throwing TechniquesJuan Jose Opazo Carvajal100% (1)
- Family Planning Methods - LatestДокумент59 страницFamily Planning Methods - LatestGenevieve VillaflorОценок пока нет
- Newborn Assessment, Apgar & Ballard Scoring NotesДокумент3 страницыNewborn Assessment, Apgar & Ballard Scoring NotesAshitakaОценок пока нет
- Hyper Bilirubin Emi AДокумент29 страницHyper Bilirubin Emi ANinz NunezОценок пока нет
- Blood Transfusion FinalДокумент8 страницBlood Transfusion FinalejkohОценок пока нет
- Yehuda Berg Satan PDFДокумент77 страницYehuda Berg Satan PDFOswaldo Archundia100% (7)
- Anorectal Malformations: Presented by Khushveer KaurДокумент91 страницаAnorectal Malformations: Presented by Khushveer KaurKataria DavinОценок пока нет
- Play TherapyДокумент6 страницPlay TherapyNylia AtibiОценок пока нет
- Surgical Instruments: Grasping and Holding Retracting and Exposing Cutting and Dissecting Clamping and OccludingДокумент55 страницSurgical Instruments: Grasping and Holding Retracting and Exposing Cutting and Dissecting Clamping and OccludingNylia AtibiОценок пока нет
- LTE 3GPP Band13 Test Entrance CriteriaДокумент130 страницLTE 3GPP Band13 Test Entrance CriteriaBuchi Reddy0% (1)
- Neonatal Hypoglycemia APNECДокумент26 страницNeonatal Hypoglycemia APNECyumicheongОценок пока нет
- Planet Earth: Its Propeties To Support LifeДокумент27 страницPlanet Earth: Its Propeties To Support LifegillianeОценок пока нет
- Induction of Labour Techniq SAДокумент18 страницInduction of Labour Techniq SAPujanaWiaktaОценок пока нет
- Neonatal SepsisДокумент26 страницNeonatal SepsisKimbek BuangkeОценок пока нет
- HypoglycaemiaДокумент36 страницHypoglycaemiaAwatef AbushhiwaОценок пока нет
- Photography Techniques (Intermediate)Документ43 страницыPhotography Techniques (Intermediate)Truc Nguyen100% (2)
- Guidelines For Newborn Hearing Screening and EvaluationДокумент2 страницыGuidelines For Newborn Hearing Screening and EvaluationAileen A. MonaresОценок пока нет
- Bams 1st Rachna Sharir Joints and Their Classification 16-05-2020Документ15 страницBams 1st Rachna Sharir Joints and Their Classification 16-05-2020Sanjana SajjanarОценок пока нет
- The Images Are Belongs To The Rightful Owners.: Governor Panotes Avenue, Daet, Camarines NorteДокумент10 страницThe Images Are Belongs To The Rightful Owners.: Governor Panotes Avenue, Daet, Camarines NorteNylia AtibiОценок пока нет
- Scattered Pearls: Selected Sayings and Anecdotes of The Illustrious AuliyaaДокумент103 страницыScattered Pearls: Selected Sayings and Anecdotes of The Illustrious AuliyaaYeye17100% (1)
- L15 - Parallel Magnetic CircuitsДокумент6 страницL15 - Parallel Magnetic CircuitsParikshit MishraОценок пока нет
- Case Study Congenital HyperthyroidismДокумент10 страницCase Study Congenital HyperthyroidismCamille CaraanОценок пока нет
- Child's HerniaДокумент13 страницChild's HerniaKreshnik HAJDARIОценок пока нет
- Sr. IBS DAS Consultant EngineerДокумент4 страницыSr. IBS DAS Consultant EngineerMohamed KamalОценок пока нет
- Neonatal JaundiceДокумент48 страницNeonatal JaundiceRemy MartinsОценок пока нет
- Angelic - Doc - Neonatal JaundiceДокумент16 страницAngelic - Doc - Neonatal JaundiceAngy100% (5)
- CASE REPORT - Syphilis in PregnancyДокумент28 страницCASE REPORT - Syphilis in PregnancymuhammadrubaiОценок пока нет
- Fundal Height ScreeningДокумент10 страницFundal Height ScreeningDr_Soranus100% (1)
- Neonatal ResuscitationДокумент5 страницNeonatal Resuscitationabdirahiim ahmedОценок пока нет
- Febrile Seizure Case FileДокумент4 страницыFebrile Seizure Case Filehttps://medical-phd.blogspot.comОценок пока нет
- Pre Natal Care Book BasedДокумент9 страницPre Natal Care Book BasedAngelaTrinidadОценок пока нет
- Case Scenario Pre Natal - FinalДокумент6 страницCase Scenario Pre Natal - Finalgwyne laguardiaОценок пока нет
- Seminar 3 ImmunizationДокумент42 страницыSeminar 3 ImmunizationRajhmuniran KandasamyОценок пока нет
- Case Study in PICUДокумент13 страницCase Study in PICUKeevin BalastonОценок пока нет
- Examination of Newborn Physical Examination Include The FollowingДокумент34 страницыExamination of Newborn Physical Examination Include The FollowingZimm Rrrr100% (2)
- Paediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota KinabaluДокумент41 страницаPaediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota Kinabaluarnol3090Оценок пока нет
- Atresia EsophagusДокумент6 страницAtresia EsophagusPPN38 UNPADОценок пока нет
- Pediatric Abdominal Assessment: Hind Al-SuwaisДокумент20 страницPediatric Abdominal Assessment: Hind Al-SuwaisHINDОценок пока нет
- II. General and Specific ObjectivesДокумент5 страницII. General and Specific ObjectivesRae Marie AquinoОценок пока нет
- PROM SANJIDA FInal 2Документ32 страницыPROM SANJIDA FInal 2Saiful islam RonyОценок пока нет
- Labor and Delivery 34: Removing OvariesДокумент3 страницыLabor and Delivery 34: Removing OvariesDianneОценок пока нет
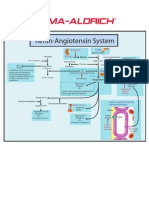
- Renin-Angiotensin SystemДокумент1 страницаRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Lens Related GlaucomaДокумент19 страницLens Related GlaucomaUsama ButtОценок пока нет
- Harika Priyanka. K Asst. Professor AconДокумент30 страницHarika Priyanka. K Asst. Professor AconArchana MoreyОценок пока нет
- Normal Growth and DevelopmentДокумент8 страницNormal Growth and DevelopmentMonaliza ZahariОценок пока нет
- 1 - Fetal Physiology and The Transition To Extrauterine LifeДокумент13 страниц1 - Fetal Physiology and The Transition To Extrauterine LifeRonaldo Pineda WieselbergОценок пока нет
- Per Vaginal Bleeding in PregnancyДокумент33 страницыPer Vaginal Bleeding in PregnancyKai Wei LimОценок пока нет
- Amniotic Fluid EmbolismДокумент34 страницыAmniotic Fluid EmbolismReygie MataОценок пока нет
- Cervical Insufficiency + Cord PresentationДокумент2 страницыCervical Insufficiency + Cord PresentationMSОценок пока нет
- Abnormal LabourДокумент12 страницAbnormal Labourabidul hoqueОценок пока нет
- Fluid Management in MalnutritionДокумент30 страницFluid Management in MalnutritionCHALIE MEQUОценок пока нет
- 56 Ambiguous GenitaliaДокумент8 страниц56 Ambiguous GenitalianasibdinОценок пока нет
- Allergic Rhinitis in ChildrenДокумент7 страницAllergic Rhinitis in ChildrenTina MorleyОценок пока нет
- Physiologic Changes PregnancyДокумент53 страницыPhysiologic Changes PregnancyDeedong Zydee100% (1)
- Birth AsphyxiaДокумент20 страницBirth Asphyxiainne_fОценок пока нет
- 19.neonatal JaundiceДокумент42 страницы19.neonatal JaundiceWilhellmuss MaukaОценок пока нет
- Cystocele & RectoceleДокумент26 страницCystocele & RectoceleAlmasОценок пока нет
- PARTOGRAMДокумент17 страницPARTOGRAMKrutthivaasa PriyaОценок пока нет
- Nursing Care PlanДокумент6 страницNursing Care PlanJohann OrtizОценок пока нет
- Third Stage of Labour (Normal & Abnormal) : Dr. Abdalla H. Elsadig MDДокумент29 страницThird Stage of Labour (Normal & Abnormal) : Dr. Abdalla H. Elsadig MDAsogaa MeteranОценок пока нет
- HydrocephalusДокумент36 страницHydrocephalusRushdaОценок пока нет
- Common Problems in NeonatesДокумент73 страницыCommon Problems in NeonatesWan FaizuddinОценок пока нет
- Maisel S 2012Документ5 страницMaisel S 2012marsyaОценок пока нет
- Amniotic Band SyndromeДокумент47 страницAmniotic Band SyndromeNazrul Islam JhinukОценок пока нет
- Ophthalmic Nursing EthicsДокумент29 страницOphthalmic Nursing Ethicsgideon A. owusuОценок пока нет
- Discharge Summary PDFДокумент2 страницыDischarge Summary PDFbalab2311Оценок пока нет
- Fetal Growth Restriction - ACOG 2019Документ23 страницыFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaОценок пока нет
- 16 Amniotic Fluid EmbolismДокумент46 страниц16 Amniotic Fluid EmbolismAhmed TarigОценок пока нет
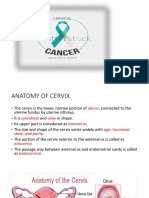
- Cervical CancerДокумент62 страницыCervical CancerRitaLakhaniОценок пока нет
- Intrauterine Growth RestrictionДокумент3 страницыIntrauterine Growth RestrictionShofiKhaqulIlmyОценок пока нет
- Hiatal Hernia: BY MR, Vinay KumarДокумент27 страницHiatal Hernia: BY MR, Vinay KumarVinay KumarОценок пока нет
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- CHN Ailyn and Lai& RealДокумент6 страницCHN Ailyn and Lai& RealNylia AtibiОценок пока нет
- CHNДокумент3 страницыCHNNylia AtibiОценок пока нет
- Case StudyДокумент11 страницCase StudyNylia AtibiОценок пока нет
- QuestionsДокумент10 страницQuestionsNylia AtibiОценок пока нет
- BurnsДокумент57 страницBurnsNylia AtibiОценок пока нет
- Xii. Miswa Con Patola: Iii. Baby Mojos in Rolled Oats BreadingДокумент10 страницXii. Miswa Con Patola: Iii. Baby Mojos in Rolled Oats BreadingNylia AtibiОценок пока нет
- Interpersonal Theory Harry Stack Sullivan-Interpersonal Relationship and MilieuДокумент1 страницаInterpersonal Theory Harry Stack Sullivan-Interpersonal Relationship and MilieuNylia AtibiОценок пока нет
- Ngcwalisa Amanda Jama Aurene Wilford Lyn Haskins Anna Coutsoudis Lenore Spies Christiane Horwood Download CitationДокумент1 страницаNgcwalisa Amanda Jama Aurene Wilford Lyn Haskins Anna Coutsoudis Lenore Spies Christiane Horwood Download CitationNylia AtibiОценок пока нет
- Educational Tool On Complementary Feeding For Infants: Basis For Maternal Role EnhancementДокумент13 страницEducational Tool On Complementary Feeding For Infants: Basis For Maternal Role EnhancementNylia AtibiОценок пока нет
- Drug Study NubainДокумент2 страницыDrug Study NubainNylia Atibi100% (1)
- Diagnosing DDHДокумент3 страницыDiagnosing DDHNylia AtibiОценок пока нет
- DocumentДокумент41 страницаDocumentNylia AtibiОценок пока нет
- Movie Review Con Case Study: Prepared By: Ailyn D. IbitaДокумент12 страницMovie Review Con Case Study: Prepared By: Ailyn D. IbitaNylia AtibiОценок пока нет
- MABINI COLLEGES Shall Cultivate A CULTURE of EXCELLENCE in Education.Документ22 страницыMABINI COLLEGES Shall Cultivate A CULTURE of EXCELLENCE in Education.Nylia AtibiОценок пока нет
- Anorexia Vs BulimiaДокумент19 страницAnorexia Vs BulimiaNylia AtibiОценок пока нет
- Nursing Care Plan in Sanke Bite and PyomyositisДокумент2 страницыNursing Care Plan in Sanke Bite and PyomyositisNylia AtibiОценок пока нет
- Diagnostic TestДокумент12 страницDiagnostic TestNylia AtibiОценок пока нет
- DrugДокумент39 страницDrugNylia AtibiОценок пока нет
- Lung CenterДокумент4 страницыLung CenterNylia AtibiОценок пока нет
- Care Plans: o o o o o o o o o o o o o o o o o oДокумент12 страницCare Plans: o o o o o o o o o o o o o o o o o oNylia AtibiОценок пока нет
- Assessment Diagnosis Planning Implementation Evaluation Case: Amoebiasis Subjective:" Madalas Po AkongДокумент47 страницAssessment Diagnosis Planning Implementation Evaluation Case: Amoebiasis Subjective:" Madalas Po AkongNylia AtibiОценок пока нет
- NicarДокумент10 страницNicarNylia AtibiОценок пока нет
- MABINI COLLEGES Shall Cultivate A CULTURE of EXCELLENCE in Education.Документ22 страницыMABINI COLLEGES Shall Cultivate A CULTURE of EXCELLENCE in Education.Nylia AtibiОценок пока нет
- DocumentДокумент10 страницDocumentNylia AtibiОценок пока нет
- HellforgedДокумент89 страницHellforgedBrian Rae100% (1)
- Math Diagnostic ExamДокумент4 страницыMath Diagnostic ExamMananquil JeromeОценок пока нет
- Density-Based Methods: DBSCAN: Density-Based Clustering Based On Connected Regions With High DensityДокумент3 страницыDensity-Based Methods: DBSCAN: Density-Based Clustering Based On Connected Regions With High DensityKingzlynОценок пока нет
- (Rect-15) Experimental Study On Partial Replacement of Cement With Coconut Shell Ash in ConcreteДокумент3 страницы(Rect-15) Experimental Study On Partial Replacement of Cement With Coconut Shell Ash in Concretefrancis dimakilingОценок пока нет
- AS-Interface Devices: (Slave Modules)Документ48 страницAS-Interface Devices: (Slave Modules)Muhamad PriyatnaОценок пока нет
- Classic Plan: Dog/Cat BedДокумент3 страницыClassic Plan: Dog/Cat BedRobson DiasОценок пока нет
- EOCR 종합 EN 2015 PDFДокумент228 страницEOCR 종합 EN 2015 PDFShubhankar KunduОценок пока нет
- SMA - Core 1 - IEC62109-2 - 0 Test ReportДокумент6 страницSMA - Core 1 - IEC62109-2 - 0 Test ReportFurqan HamidОценок пока нет
- Qualitest Canada BrochureДокумент7 страницQualitest Canada BrochureBala SingamОценок пока нет
- Linear Predictor: Nature of Linear PredictionДокумент9 страницLinear Predictor: Nature of Linear PredictionkvОценок пока нет
- NHouse SelfBuilder Brochure v2 Jan19 LowresДокумент56 страницNHouse SelfBuilder Brochure v2 Jan19 LowresAndrew Richard ThompsonОценок пока нет
- Appetizer Summative TestДокумент36 страницAppetizer Summative TestArgelynPadolinaPedernalОценок пока нет
- EclipseДокумент6 страницEclipsetoncipОценок пока нет
- Dead Zone I Air AgeДокумент7 страницDead Zone I Air AgeJaponec PicturesОценок пока нет
- Reflection in SystemsДокумент1 страницаReflection in SystemsGeraldine PadillaОценок пока нет
- National Railway Museum Annual Review 04-05Документ40 страницNational Railway Museum Annual Review 04-05sol.loredo1705530Оценок пока нет
- AN-PFC-TDA 4863-3 Calculation-Tool For PFC-Preconverter Using TDA 4863Документ9 страницAN-PFC-TDA 4863-3 Calculation-Tool For PFC-Preconverter Using TDA 4863NaciConSolОценок пока нет
- WPP Jak Campus - Defect All Level - 18042023Документ15 страницWPP Jak Campus - Defect All Level - 18042023bbm FebriОценок пока нет
- Solid State Controller of Drives - ExperimentДокумент37 страницSolid State Controller of Drives - ExperimentRakesh Singh LodhiОценок пока нет
- Smart Dust Technology Seminar ReportДокумент32 страницыSmart Dust Technology Seminar ReportSushan Upadhyay67% (3)
- NTDCДокумент8 страницNTDCjaved_hanifОценок пока нет