Вам также может понравиться
- Form-1-Medical-Form-Back-to-back 2023-04-23 06 - 10 - 49Документ2 страницыForm-1-Medical-Form-Back-to-back 2023-04-23 06 - 10 - 49Climaco EdwinОценок пока нет
- Pediatric Intake Form SampleДокумент10 страницPediatric Intake Form SampleТравма ЮніверсумОценок пока нет
- Medical Certificate of Athlete: To Whom It May ConcernДокумент3 страницыMedical Certificate of Athlete: To Whom It May ConcernRoderick CruzОценок пока нет
- Maternal & Child Health BookletДокумент17 страницMaternal & Child Health BookletAtina LavadiaОценок пока нет
- 130 Physicians-Report 7-21-2023Документ2 страницы130 Physicians-Report 7-21-2023medisnadaОценок пока нет
- Physician Verified Medical HistoryДокумент2 страницыPhysician Verified Medical HistoryHoracio RubioОценок пока нет
- Health and Medical Certificate 3Документ1 страницаHealth and Medical Certificate 3Danilo P. PancitoОценок пока нет
- BSP-Medical FormДокумент1 страницаBSP-Medical FormNyleg Aicilag100% (2)
- AHG Health & Medical FormsДокумент12 страницAHG Health & Medical FormsAnonymous 2buCBbFОценок пока нет
- Medical Form For Grade 7 12Документ3 страницыMedical Form For Grade 7 12Deonna Angeline100% (1)
- Dermatology History and Examination FormДокумент4 страницыDermatology History and Examination FormЂорђеОценок пока нет
- Pidsr CifДокумент17 страницPidsr CifAbraham Asto100% (4)
- Medical Health RecordДокумент1 страницаMedical Health RecordNikay SerdeñaОценок пока нет
- Surgery Admission 2014Документ2 страницыSurgery Admission 2014Lisa VaughnОценок пока нет
- Form 1 Medical Form Back To BackДокумент2 страницыForm 1 Medical Form Back To BackMaico ReyesОценок пока нет
- Botulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Документ18 страницBotulism Toolkit: Emergency Recognition, Response and Anti Terrorism Training Associates (ERRATA, LLC.)Joko YantoОценок пока нет
- Antipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Документ2 страницыAntipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Chlong ArtuzОценок пока нет
- Pre-Employment Medical FormsДокумент8 страницPre-Employment Medical Formsnot your medz duranОценок пока нет
- CT Screening FormДокумент1 страницаCT Screening FormJuliano PachecoОценок пока нет
- Assessment Tool of Mu SysДокумент60 страницAssessment Tool of Mu SysBeulah DasariОценок пока нет
- Operating Room NotesДокумент35 страницOperating Room NotesMagdaraog Gabrielle A.Оценок пока нет
- Natoza Medical Form For Grade 7 12Документ3 страницыNatoza Medical Form For Grade 7 12Deonna AngelineОценок пока нет
- Pediatrician Report: Questions Relating To Proposed InsuredДокумент2 страницыPediatrician Report: Questions Relating To Proposed InsuredSincerely ReynОценок пока нет
- Medical Pro Form AДокумент5 страницMedical Pro Form Atanujchopra1Оценок пока нет
- Medical Disbursement Monitoring FormДокумент2 страницыMedical Disbursement Monitoring Formgenalcantara83Оценок пока нет
- Medical QuestionnaireДокумент2 страницыMedical QuestionnaireNyambod NestorОценок пока нет
- My Personal Health RecordДокумент2 страницыMy Personal Health RecordKimmi Joy BakerОценок пока нет
- Consent Form - Pfizer-Biontech Covid-19 VaccineДокумент2 страницыConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaОценок пока нет
- Medical Report: Reason RequestedДокумент4 страницыMedical Report: Reason RequestedWebmaster0% (1)
- My O&g Clerking TemplateДокумент8 страницMy O&g Clerking TemplateFarah FadzilОценок пока нет
- Parental Consent Form: To Whom It May ConcernДокумент4 страницыParental Consent Form: To Whom It May ConcernNorman PolilinОценок пока нет
- Medical History FormДокумент5 страницMedical History FormgaloperiscolОценок пока нет
- Format For Medical FitnessДокумент4 страницыFormat For Medical FitnessParas JaniОценок пока нет
- Medical PerformaДокумент5 страницMedical Performamashal naeemОценок пока нет
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusДокумент4 страницыOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjОценок пока нет
- HEALTH HISTORY GUIDE. ReviseДокумент2 страницыHEALTH HISTORY GUIDE. ReviseCathryn luv QuisidoОценок пока нет
- HH FormДокумент2 страницыHH FormStefanie Kiss-PlucasОценок пока нет
- P.A. Tool (Case Pres FINAL.)Документ23 страницыP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonОценок пока нет
- Medical FormДокумент2 страницыMedical FormAshok sankerОценок пока нет
- Medicaltests FormnДокумент1 страницаMedicaltests FormnJasanta JinorОценок пока нет
- 2009-2010 Medical Release FormДокумент2 страницы2009-2010 Medical Release FormchaclynknowsОценок пока нет
- Medical Form For All ApplicantsДокумент2 страницыMedical Form For All ApplicantsHaason TzОценок пока нет
- History TakingДокумент6 страницHistory Takingdharti daveОценок пока нет
- 2.physical E, HISTORY NCPДокумент13 страниц2.physical E, HISTORY NCPمريم حجيОценок пока нет
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientДокумент5 страницANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonОценок пока нет
- DP New Patient Form - 2023Документ5 страницDP New Patient Form - 2023cdbn2326Оценок пока нет
- 43 Laceration Suturing For AvulsionДокумент3 страницы43 Laceration Suturing For AvulsionAkash KОценок пока нет
- DR Langford1Документ8 страницDR Langford1Spencer JacksonОценок пока нет
- Health Questionnaire: Oral &maxillofacial SurgeryДокумент6 страницHealth Questionnaire: Oral &maxillofacial SurgeryPaul MathaiОценок пока нет
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDДокумент3 страницыViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaОценок пока нет
- Fitness Form & Hospital ListДокумент15 страницFitness Form & Hospital Listjohn thomasОценок пока нет
- CT Scan Ref-Brampton CivicДокумент1 страницаCT Scan Ref-Brampton CivicalikuniОценок пока нет
- 8.) Health-and-Medical-Profile Template Ver.2Документ4 страницы8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangОценок пока нет
- Obstetrics History General DataДокумент7 страницObstetrics History General DataColeen NeyraОценок пока нет
- Pedia Case ProtocolДокумент5 страницPedia Case ProtocolAllene PaderangaОценок пока нет
- Prenatal Check Up InterviewДокумент7 страницPrenatal Check Up InterviewSHIELOU LOMODОценок пока нет
- Student Physician FormДокумент1 страницаStudent Physician FormMasr RedaОценок пока нет
- Health Statement Form Medical Questionnaire (2M Up)Документ1 страницаHealth Statement Form Medical Questionnaire (2M Up)DECA HOMES YAKALОценок пока нет
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationДокумент3 страницыTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenОценок пока нет
- Jurnal Difteri English PDFДокумент9 страницJurnal Difteri English PDFLisbet Anita SimamoraОценок пока нет
- First Dengue Vaccine Goes Under Final Test in PH: Charles E. Buban Philippine Daily InquirerДокумент2 страницыFirst Dengue Vaccine Goes Under Final Test in PH: Charles E. Buban Philippine Daily Inquireryer tagalajОценок пока нет
- Surveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionДокумент28 страницSurveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDebОценок пока нет
- GBS Guideline RCOGДокумент26 страницGBS Guideline RCOGwoihonОценок пока нет
- Musana 2020 Come and See ApplicationДокумент8 страницMusana 2020 Come and See ApplicationCasey PayneОценок пока нет
- Flumist PiДокумент4 страницыFlumist Pijasonm2282Оценок пока нет
- Swine Flu & You: Questions & AnswersДокумент3 страницыSwine Flu & You: Questions & Answerssv swamyОценок пока нет
- Tetanus BrochureДокумент2 страницыTetanus BrochureOpuntia PclОценок пока нет
- Immunisation and Vaccination FormДокумент6 страницImmunisation and Vaccination FormLawrenceZengОценок пока нет
- Animal BitesДокумент5 страницAnimal BitesvyalylaОценок пока нет
- Ob Case Study - BCG Drug StudyДокумент1 страницаOb Case Study - BCG Drug StudyAngelica Rose Villegas0% (1)
- SB Cleaning Sharps GuidancesheetДокумент2 страницыSB Cleaning Sharps Guidancesheetالأغا محمد زكارنةОценок пока нет
- Toddler FinalДокумент9 страницToddler FinalVon BernalОценок пока нет
- Doh DC 2018-0142Документ2 страницыDoh DC 2018-0142vanceОценок пока нет
- HEPATITIS A (Infectious Hepatitis)Документ3 страницыHEPATITIS A (Infectious Hepatitis)Lovely Ann AyapanaОценок пока нет
- Dengue Death Case Investigation Form (CIF)Документ3 страницыDengue Death Case Investigation Form (CIF)Chamee Mallillin100% (1)
- Guideline On Bi-Annual Vitamin A Supplementation: ND NDДокумент11 страницGuideline On Bi-Annual Vitamin A Supplementation: ND NDSWAPAN KUMAR SARKARОценок пока нет
- Jurnal MorbiliДокумент8 страницJurnal MorbiliNely KeybumОценок пока нет
- Antihbs ArcДокумент6 страницAntihbs ArcYu YingОценок пока нет
- La Consolacion College Manila School of Nursing Course SyllabusДокумент4 страницыLa Consolacion College Manila School of Nursing Course SyllabusJayson Magdael SalvadorОценок пока нет
- Storage Handling ToolkitДокумент81 страницаStorage Handling ToolkitAudraОценок пока нет
- Immunization UipДокумент20 страницImmunization Uipdevesh gargОценок пока нет
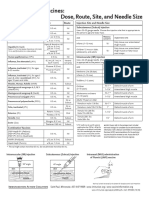
- Injection Site and Needle Size Vaccine Dose RouteДокумент1 страницаInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaОценок пока нет
- Brainstorming About Vaccines-1 1Документ6 страницBrainstorming About Vaccines-1 1api-242698568Оценок пока нет
- Vaccination Chemtrail Alerts 4-9-12Документ5 страницVaccination Chemtrail Alerts 4-9-12DrScottJohnsonTeachingsОценок пока нет
- Recommendations of The Advisory Committee On Immunization Practices (ACIP)Документ64 страницыRecommendations of The Advisory Committee On Immunization Practices (ACIP)Prabir Kumar ChatterjeeОценок пока нет
- Sub Centre Level Monitoring Checklist PHC VisitДокумент24 страницыSub Centre Level Monitoring Checklist PHC VisitVaish Navi100% (2)
- SPMC 1 PDFДокумент62 страницыSPMC 1 PDFJ.m.RahulОценок пока нет
- M Alaria in Pregnancy: Priorities For Research: ReviewДокумент12 страницM Alaria in Pregnancy: Priorities For Research: ReviewSanjana PrasadОценок пока нет
- Vaccination in PregnancyДокумент7 страницVaccination in PregnancyNoraОценок пока нет
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingОт EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingРейтинг: 4.5 из 5 звезд4.5/5 (104)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipОт EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipРейтинг: 4.5 из 5 звезд4.5/5 (1135)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissОт EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissРейтинг: 4.5 из 5 звезд4.5/5 (82)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductОт EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductРейтинг: 5 из 5 звезд5/5 (31)
- Love Yourself, Heal Your Life Workbook (Insight Guide)От EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Рейтинг: 5 из 5 звезд5/5 (40)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookОт EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookРейтинг: 3.5 из 5 звезд3.5/5 (2)
- The Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayОт EverandThe Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayОценок пока нет
- The Art of Stillness: Adventures in Going NowhereОт EverandThe Art of Stillness: Adventures in Going NowhereРейтинг: 4.5 из 5 звезд4.5/5 (69)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayОт EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayОценок пока нет
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeОт EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeРейтинг: 3.5 из 5 звезд3.5/5 (13)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouОт EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouРейтинг: 3.5 из 5 звезд3.5/5 (5)
- The Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeОт EverandThe Self-Care Solution: A Year of Becoming Happier, Healthier, and Fitter—One Month at a TimeРейтинг: 3 из 5 звезд3/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeОт EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeРейтинг: 4 из 5 звезд4/5 (3)
- What to Expect When You’re Expecting (5th Edition)От EverandWhat to Expect When You’re Expecting (5th Edition)Рейтинг: 5 из 5 звезд5/5 (1)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomОт EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomРейтинг: 4 из 5 звезд4/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthОт EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthОценок пока нет
- Calm: The Magic of Sleep: A Beside CompanionОт EverandCalm: The Magic of Sleep: A Beside CompanionРейтинг: 5 из 5 звезд5/5 (10)
- Clean Mama's Guide to a Healthy Home: The Simple, Room-by-Room Plan for a Natural HomeОт EverandClean Mama's Guide to a Healthy Home: The Simple, Room-by-Room Plan for a Natural HomeРейтинг: 5 из 5 звезд5/5 (2)