Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Educational Series in Congenital Heart DISEASE: Tetralogy of Fallot: Diagnosis To Long-Term Follow-UpДокумент15 страницEducational Series in Congenital Heart DISEASE: Tetralogy of Fallot: Diagnosis To Long-Term Follow-UpDr Mohammed Nizam UddinОценок пока нет
- A Patient Safety Checklist For The Cardiac Catheterisation LaboratoryДокумент5 страницA Patient Safety Checklist For The Cardiac Catheterisation LaboratoryKena Ben100% (1)
- Medical Surgical Nursing Pre-Test 2 RATIONALEДокумент8 страницMedical Surgical Nursing Pre-Test 2 RATIONALEBlaine ManiegoОценок пока нет
- Cardiac CatheterizationДокумент2 страницыCardiac Catheterizationjacallis50% (2)
- European Resuscitation Council and European SocietДокумент50 страницEuropean Resuscitation Council and European SocietVerinceanu AlexandruОценок пока нет
- Cardiac Catheterization Lab NurseДокумент15 страницCardiac Catheterization Lab NurseLoid Sangcha-anОценок пока нет
- Fundamentals of Nursing 1Документ6 страницFundamentals of Nursing 1Fatima Medriza DuranОценок пока нет
- Cardiac Cath Lab:: Where We Were, Where We Are and Where We Are GoingДокумент51 страницаCardiac Cath Lab:: Where We Were, Where We Are and Where We Are GoingXunyao LuОценок пока нет
- جميع اكواد منصة نفيس المنظمة للقطاع الصحي السعوديДокумент615 страницجميع اكواد منصة نفيس المنظمة للقطاع الصحي السعوديNehal ElnagarОценок пока нет
- Study This Question Med Surg FinalДокумент14 страницStudy This Question Med Surg FinalAna Gonzalez83% (6)
- OmerДокумент33 страницыOmerNoor Hasan WaheedОценок пока нет
- HTAP La VarstniciДокумент16 страницHTAP La VarstnicidanradulescuОценок пока нет
- New Right Bundle Branch Block As A CriterionДокумент3 страницыNew Right Bundle Branch Block As A CriterionNITACORDEIROОценок пока нет
- SAMPLE CV Workplace Doctors WebДокумент5 страницSAMPLE CV Workplace Doctors WebAdnan SiddiqueОценок пока нет
- Cath Lab ReportДокумент13 страницCath Lab ReportNasim AhmadОценок пока нет
- Cardiac Catheterization: Information For PatientsДокумент5 страницCardiac Catheterization: Information For PatientsgireeshsachinОценок пока нет
- Veterinary Clinics: Congenital Heart Diseases of Puppies and KittensДокумент29 страницVeterinary Clinics: Congenital Heart Diseases of Puppies and KittensPaola ChanОценок пока нет
- Medical Surgical Nursing Practice Test Part 1Документ57 страницMedical Surgical Nursing Practice Test Part 1Tina Van Winks100% (2)
- Medical Coding 1 - 2 Study GuideДокумент41 страницаMedical Coding 1 - 2 Study GuideAnthony Martinez75% (4)
- IAS AneurysmДокумент13 страницIAS AneurysmE'len HamidahОценок пока нет
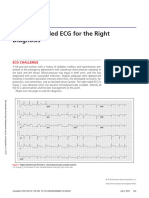
- 2018.the Right-Sided ECG For The Right DiagnosisДокумент3 страницы2018.the Right-Sided ECG For The Right DiagnosisWeila dos Santos VieiraОценок пока нет
- Differences Between Left and Right Heart Failure: Diagnosis and TreatmentДокумент118 страницDifferences Between Left and Right Heart Failure: Diagnosis and TreatmentMirza Thaariq HapsitoОценок пока нет
- Anesthesia and Anesthetic Choices Authors: Scott A Falk, MD, Lee A Fleisher, MDДокумент14 страницAnesthesia and Anesthetic Choices Authors: Scott A Falk, MD, Lee A Fleisher, MDTania Parra MoralesОценок пока нет
- Angeborene Koronarfisteln - Die Häufigste Angeborene KoronaranomalieДокумент8 страницAngeborene Koronarfisteln - Die Häufigste Angeborene KoronaranomalieCHEОценок пока нет
- ICU-ED Clinical AssignmentДокумент5 страницICU-ED Clinical AssignmentMark LiebОценок пока нет
- Coronarry Artery DiseaseДокумент24 страницыCoronarry Artery DiseaseAriess897Оценок пока нет
- Sample Magaling Med CenterДокумент44 страницыSample Magaling Med CenterDiana LiОценок пока нет
- Medical Surgical Nursing - Responses To Altered Tissue PerfusionДокумент23 страницыMedical Surgical Nursing - Responses To Altered Tissue PerfusionLouise NicoleОценок пока нет
- MO Handbook 2ndEDДокумент87 страницMO Handbook 2ndED王骏原Оценок пока нет
- CardionotesДокумент5 страницCardionotesNichole Coletta100% (1)