Вам также может понравиться
- Classification of BurnsДокумент16 страницClassification of BurnsMauricio SvОценок пока нет
- Acute Biologic CauseДокумент15 страницAcute Biologic CauseMizen ChristalОценок пока нет
- Burns and ShockДокумент13 страницBurns and Shockjames garciaОценок пока нет
- Assessment and Classification of BurnДокумент3 страницыAssessment and Classification of BurnFadila PadmariniОценок пока нет
- Classification of BurnsДокумент4 страницыClassification of BurnsErtania NirmalaОценок пока нет
- Burns: Major and Minor BurnsДокумент25 страницBurns: Major and Minor BurnsTrisha TannerОценок пока нет
- Burns: Dr. Iye D. Otigba-KolawoleДокумент37 страницBurns: Dr. Iye D. Otigba-KolawoleMaryОценок пока нет
- Clinical Review - FullДокумент5 страницClinical Review - FullAnen LightОценок пока нет
- Gran QuemadoДокумент11 страницGran QuemadoLisbeth Gaete CórdovaОценок пока нет
- 1st Congress of Pharmaceutical Students AssociationДокумент24 страницы1st Congress of Pharmaceutical Students AssociationEcaterinaGuţuţuiОценок пока нет
- Picu Protocols-Dr - Mohan Shenoy - 2.8.2010Документ117 страницPicu Protocols-Dr - Mohan Shenoy - 2.8.2010Aimhigh_PPMОценок пока нет
- Salinan Terjemahan 91287 - Artikel 4 p2k2Документ12 страницSalinan Terjemahan 91287 - Artikel 4 p2k2anon_659186730Оценок пока нет
- 5 Chemical Burn - ManuscriptДокумент7 страниц5 Chemical Burn - Manuscriptkint manlangitОценок пока нет
- Burn Ulcer Management: Salafudin YusraДокумент44 страницыBurn Ulcer Management: Salafudin Yusraarief AnwarОценок пока нет
- Vigani2017 1Документ15 страницVigani2017 1Alexandra AvanuОценок пока нет
- BURNДокумент39 страницBURNMuhammad MakkiОценок пока нет
- Case Pres PartДокумент12 страницCase Pres PartJeannezelle Anne Mariz GazaОценок пока нет
- Modern Aspects of Burn Injury ImmunopathogenesisДокумент12 страницModern Aspects of Burn Injury ImmunopathogenesisYohana Elisabeth GultomОценок пока нет
- Burn Injuries and Their Medico-legal AspectsДокумент5 страницBurn Injuries and Their Medico-legal AspectsNIKITAОценок пока нет
- Advances A. BackgroundДокумент24 страницыAdvances A. Backgroundalistia andiniОценок пока нет
- 1 s2.0 S0263931921002404 MainДокумент8 страниц1 s2.0 S0263931921002404 MainMarina UlfaОценок пока нет
- About BurnsДокумент14 страницAbout BurnsSamОценок пока нет
- BurnДокумент11 страницBurnsofea zamriОценок пока нет
- Types of Burns ArticleДокумент7 страницTypes of Burns ArticleSeltri 'ceti' SeptianiОценок пока нет
- Burn Rehabiliation GuideДокумент7 страницBurn Rehabiliation GuideJia MedinaОценок пока нет
- Burns 3Документ31 страницаBurns 3Reann LeeОценок пока нет
- Burns Care GuideДокумент106 страницBurns Care GuideShahini PrajapatiОценок пока нет
- NCM 106 BurnsДокумент9 страницNCM 106 BurnsJudeLaxОценок пока нет
- Side-Effects of Topical Steroids: A Long Overdue Revisit: Review ArticleДокумент10 страницSide-Effects of Topical Steroids: A Long Overdue Revisit: Review ArticleVidini Kusuma AjiОценок пока нет
- Types and Causes of Burns ExplainedДокумент4 страницыTypes and Causes of Burns Explainedgreshel254981Оценок пока нет
- Pediatric Burn Emergency CareДокумент18 страницPediatric Burn Emergency CareItalo J B DuarteОценок пока нет
- Environmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesДокумент48 страницEnvironmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesJay MОценок пока нет
- burnsДокумент26 страницburnsgemergencycareОценок пока нет
- Case Study BurnДокумент3 страницыCase Study Burn去約翰Оценок пока нет
- Management and Treatment of Burn WoundДокумент5 страницManagement and Treatment of Burn WoundTaqi MehdiОценок пока нет
- Burns in Small Animals - WSAVA2013 - VINДокумент4 страницыBurns in Small Animals - WSAVA2013 - VINApra ShahiОценок пока нет
- BurnsДокумент57 страницBurnsNylia AtibiОценок пока нет
- Pamantasan NG Lungsod NG Maynila: (University of The City of Manila)Документ23 страницыPamantasan NG Lungsod NG Maynila: (University of The City of Manila)Em Hernandez AranaОценок пока нет
- Burn Injury PDFДокумент82 страницыBurn Injury PDFFirras Salsabila100% (1)
- Peripheral Mechanisms of Burn Injury Associated PainДокумент10 страницPeripheral Mechanisms of Burn Injury Associated Pain小次郎 佐々木Оценок пока нет
- Jemal Yimam Jibril Berhanu Kalkidan Zenebe: Presented byДокумент57 страницJemal Yimam Jibril Berhanu Kalkidan Zenebe: Presented byVincent SerОценок пока нет
- PsoriasisPaperДокумент8 страницPsoriasisPaperJayjay TillieОценок пока нет
- Prolonged SteroidДокумент10 страницProlonged Steroidindah ayuОценок пока нет
- BurnsДокумент5 страницBurnsaster27Оценок пока нет
- Añosa Caballo - First Aid For Burns HandoutДокумент21 страницаAñosa Caballo - First Aid For Burns HandoutMa. Ferimi Gleam BajadoОценок пока нет
- DR Samson Burn 2Документ85 страницDR Samson Burn 2Bogale DegefaОценок пока нет
- Burns: Samir Jabaiti, MD, FRCS University of JordanДокумент7 страницBurns: Samir Jabaiti, MD, FRCS University of JordanSuhaeb AlmarafyОценок пока нет
- Burn Care Procedures: Wound EvaluationДокумент34 страницыBurn Care Procedures: Wound EvaluationHafiz KhairunОценок пока нет
- Toxic Epidermal Necrolysis: A Paradigm of Critical IllnessДокумент10 страницToxic Epidermal Necrolysis: A Paradigm of Critical IllnessViolett LiebeОценок пока нет
- M8 BurnsДокумент12 страницM8 BurnsFRANCESCA MARIE MIRANDAОценок пока нет
- BURN NoteДокумент3 страницыBURN NoteClarence BravioОценок пока нет
- The White Army-BurnsДокумент69 страницThe White Army-BurnsVishnu PriyaОценок пока нет
- Thermal Burns: PrinciplesДокумент11 страницThermal Burns: PrinciplesHafiz KhairunОценок пока нет
- Burn management guideДокумент36 страницBurn management guideAshok SabalОценок пока нет
- Evaluation and Management of Sunburn: Roshni PR, Remya Reghu, Meenu Vijayan and Parvati KrishnanДокумент4 страницыEvaluation and Management of Sunburn: Roshni PR, Remya Reghu, Meenu Vijayan and Parvati KrishnanMasri RaisОценок пока нет
- PV1211 Frantz CEДокумент6 страницPV1211 Frantz CERoman MamunОценок пока нет
- Holaday1997 ResilienceДокумент11 страницHoladay1997 ResilienceRakha 69Оценок пока нет
- RU BurnsДокумент18 страницRU BurnsDanah CandelarioОценок пока нет
- ECG Made EasyДокумент30 страницECG Made EasyMohan KrishabiОценок пока нет
- Peripheral NeuropathyДокумент13 страницPeripheral NeuropathyMohan KrishabiОценок пока нет
- Entrapment NeuropathyДокумент10 страницEntrapment NeuropathyMohan KrishabiОценок пока нет
- Types of HeadacheДокумент1 страницаTypes of HeadacheMohan KrishabiОценок пока нет
- Age Related Decresed TestosteroneДокумент1 страницаAge Related Decresed TestosteroneMohan KrishabiОценок пока нет
- CN PoliomyelitisДокумент9 страницCN PoliomyelitisMohan KrishabiОценок пока нет
- Alzheimer's DiseaseДокумент4 страницыAlzheimer's DiseaseMohan KrishabiОценок пока нет
- Quick Facts About Corona VirusДокумент1 страницаQuick Facts About Corona VirusMohan KrishabiОценок пока нет
- Myotonic Dystrophy Type I (Steinert's Disease)Документ3 страницыMyotonic Dystrophy Type I (Steinert's Disease)Mohan KrishabiОценок пока нет
- Pyloric StenosisДокумент1 страницаPyloric StenosisMohan KrishabiОценок пока нет
- Acute Kidney InjuryДокумент1 страницаAcute Kidney InjuryMohan KrishabiОценок пока нет
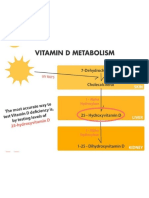
- Vitamin D MechanismДокумент1 страницаVitamin D MechanismMohan KrishabiОценок пока нет
- Antidiabetic Drugs and Action On OrgansДокумент1 страницаAntidiabetic Drugs and Action On OrgansMohan KrishabiОценок пока нет
- Pathophysiology of Pulmonary EmbolismДокумент1 страницаPathophysiology of Pulmonary EmbolismMohan Krishabi100% (1)
- Integummentry System Physiology..Документ1 страницаIntegummentry System Physiology..Mohan KrishabiОценок пока нет
- Bone NanoanatomyДокумент1 страницаBone NanoanatomyMohan KrishabiОценок пока нет
- Reproductive System PhysiologyДокумент1 страницаReproductive System PhysiologyMohan KrishabiОценок пока нет
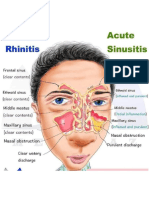
- Allergic Rhinitis Vs Acute SinusitisДокумент1 страницаAllergic Rhinitis Vs Acute SinusitisMohan KrishabiОценок пока нет
- Coma MechanismДокумент1 страницаComa MechanismMohan KrishabiОценок пока нет
- Weber and Rinne TestДокумент1 страницаWeber and Rinne TestMohan KrishabiОценок пока нет
- Events in HearingДокумент1 страницаEvents in HearingMohan KrishabiОценок пока нет
- Cystic Fibrosis SymptomsДокумент1 страницаCystic Fibrosis SymptomsMohan KrishabiОценок пока нет
- Sciatica ExerciseДокумент1 страницаSciatica ExerciseMohan KrishabiОценок пока нет
- Trigeminal Nerve CourseДокумент1 страницаTrigeminal Nerve CourseMohan KrishabiОценок пока нет
- On Examination Full BodyДокумент1 страницаOn Examination Full BodyMohan KrishabiОценок пока нет
- Vagus and Accessory Nerve CourseДокумент1 страницаVagus and Accessory Nerve CourseMohan KrishabiОценок пока нет
- Effects of HeraineДокумент2 страницыEffects of HeraineMohan KrishabiОценок пока нет
- Multiple SclerosisДокумент1 страницаMultiple SclerosisMohan KrishabiОценок пока нет
- Power and Sample Size Calculation GuideДокумент13 страницPower and Sample Size Calculation Guidefranckiko2Оценок пока нет
- Lumbosacral Plexus # 6Документ6 страницLumbosacral Plexus # 6Arcel De Luca G.Оценок пока нет
- Workbook 2Документ82 страницыWorkbook 2Jobelle Cariño Resuello67% (3)
- Advocacy PaperДокумент3 страницыAdvocacy Paperapi-478583234Оценок пока нет
- Japanese EncephalitisДокумент5 страницJapanese EncephalitisBorja MelaraОценок пока нет
- Wojejuterer Health Assessment in Nursing 5th Edition PupegДокумент3 страницыWojejuterer Health Assessment in Nursing 5th Edition Pupegace Decla100% (1)
- Hubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020Документ6 страницHubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020nur halimaОценок пока нет
- Final Thesis Abdi Majid Mohamed HassanДокумент26 страницFinal Thesis Abdi Majid Mohamed HassanAbdi Majid Mohamed Hassan100% (1)
- Practical Applications of Manual Lymphatic TherapyДокумент103 страницыPractical Applications of Manual Lymphatic TherapyTito Alho100% (1)
- Effectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyДокумент8 страницEffectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyIJAR JOURNALОценок пока нет
- Cambridge OET AnswersДокумент11 страницCambridge OET AnswersNimraj Patel100% (3)
- ProP - Differentiating Nuclear Sclerosis From CataractsДокумент6 страницProP - Differentiating Nuclear Sclerosis From CataractsDita TaepangОценок пока нет
- 04 Hemoglobin ThalassemiasДокумент37 страниц04 Hemoglobin ThalassemiasBianca Ocampo100% (1)
- Katzung - Basic and Clinical Pharmacology 12th Edition (2012) PDFДокумент8 страницKatzung - Basic and Clinical Pharmacology 12th Edition (2012) PDFAl Aleem0% (2)
- DR Sumit Garg Projec-IECДокумент10 страницDR Sumit Garg Projec-IECkamlesh yadavОценок пока нет
- Drugs for Cough, Bronchial Asthma and InflammationДокумент47 страницDrugs for Cough, Bronchial Asthma and InflammationNavlika DuttaОценок пока нет
- Swallowing Rehabilitation Following Spinal Injury A Case SeriesДокумент12 страницSwallowing Rehabilitation Following Spinal Injury A Case SeriesniekoОценок пока нет
- A Study To Assess The Knowledge, Attitude and Practice of Health Workers Regarding Nosocomial Infection at Selected Hospitals of Birtamode Municipality, JhapaДокумент5 страницA Study To Assess The Knowledge, Attitude and Practice of Health Workers Regarding Nosocomial Infection at Selected Hospitals of Birtamode Municipality, JhapaIJCRM Research JournalОценок пока нет
- Fu-Chan WeiДокумент2 страницыFu-Chan WeiRoberto AlvaradoОценок пока нет
- Role of Consent in Medical PracticeДокумент8 страницRole of Consent in Medical Practiceshweta SharmaОценок пока нет
- Modern Management of Anal FistulaДокумент11 страницModern Management of Anal FistulaMayerlin CalvacheОценок пока нет
- What Is GerontologyДокумент44 страницыWhat Is GerontologyPalwasha Khan100% (1)
- Safe syringe pump practice for patient careДокумент3 страницыSafe syringe pump practice for patient careDian NoveraОценок пока нет
- Caesarean Section Performing Caesarean SectionДокумент13 страницCaesarean Section Performing Caesarean SectionBlablabla BlablablaОценок пока нет
- Hospitalized for Bleeding Peptic UlcerДокумент53 страницыHospitalized for Bleeding Peptic UlcerHoney Lyn AlebioОценок пока нет
- Question 1Документ25 страницQuestion 1Anonymous 1T0qSzPt1PОценок пока нет
- Anadin Extra TabletsДокумент6 страницAnadin Extra TabletsZeynep AkıОценок пока нет
- Designer No Auxilio Ao Cobate Da Covid 19Документ1 страницаDesigner No Auxilio Ao Cobate Da Covid 19suzy luaОценок пока нет
- Medical Surgical Nursing Practice Test Part 1Документ15 страницMedical Surgical Nursing Practice Test Part 1cleznielОценок пока нет
- Cipp 2015 AbstractsДокумент88 страницCipp 2015 AbstractsBuyanaaRise100% (2)
- 10 Anti InfectivesДокумент29 страниц10 Anti InfectivesFrançoise BОценок пока нет