Вам также может понравиться
- RC Columns For Construction: Existing Culvert Location 900 MM Dia. CULVERTДокумент1 страницаRC Columns For Construction: Existing Culvert Location 900 MM Dia. CULVERTmax viejaОценок пока нет
- GRasdДокумент11 страницGRasdmax viejaОценок пока нет
- Perspective A (Front) Perspective B (Rear) : Epoxy Paint Finish (Gray)Документ2 страницыPerspective A (Front) Perspective B (Rear) : Epoxy Paint Finish (Gray)max viejaОценок пока нет
- PWD Ramp LayoutДокумент3 страницыPWD Ramp Layoutmax viejaОценок пока нет
- Lavatory Counter and Hanging CabinetДокумент3 страницыLavatory Counter and Hanging Cabinetmax viejaОценок пока нет
- Side View A 2: Second FloorДокумент3 страницыSide View A 2: Second Floormax viejaОценок пока нет
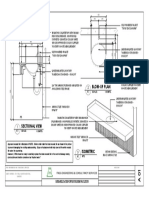
- Blow-Up Plan: FNGG Engineering and Consultancy Services RevisionsДокумент1 страницаBlow-Up Plan: FNGG Engineering and Consultancy Services Revisionsmax viejaОценок пока нет
- Blow-Up Plan: FNGG Engineering and Consultancy Services RevisionsДокумент1 страницаBlow-Up Plan: FNGG Engineering and Consultancy Services Revisionsmax viejaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Chiraghe Roshan Wa Amali Taweel - Nasir Khusrau PDFДокумент59 страницChiraghe Roshan Wa Amali Taweel - Nasir Khusrau PDFJuzer Songerwala100% (1)
- Awakening The Journalism Skills of High School StudentsДокумент3 страницыAwakening The Journalism Skills of High School StudentsMaricel BernalОценок пока нет
- Occ ST 1Документ3 страницыOcc ST 1Rona Marie BulaongОценок пока нет
- 08 Night 09 Days Ujjain & Omkareshwar Tour Package - Travel HuntДокумент5 страниц08 Night 09 Days Ujjain & Omkareshwar Tour Package - Travel HuntsalesОценок пока нет
- Michael Parenti - The Demonization of Slobodan MilosevicДокумент9 страницMichael Parenti - The Demonization of Slobodan MilosevicRicardo Castro Camba100% (1)
- HSE Matrix PlanДокумент5 страницHSE Matrix Planवात्सल्य कृतार्थ100% (1)
- Hanssen, Eirik.Документ17 страницHanssen, Eirik.crazijoeОценок пока нет
- Present Tenses ReviewДокумент6 страницPresent Tenses ReviewRamona DinuОценок пока нет
- Caisley, Robert - KissingДокумент53 страницыCaisley, Robert - KissingColleen BrutonОценок пока нет
- Thermal (TE-411,412,413,414,511)Документ25 страницThermal (TE-411,412,413,414,511)nved01Оценок пока нет
- Cloze Tests 2Документ8 страницCloze Tests 2Tatjana StijepovicОценок пока нет
- Elements of Visual Design in The Landscape - 26.11.22Документ15 страницElements of Visual Design in The Landscape - 26.11.22Delnard OnchwatiОценок пока нет
- LabДокумент11 страницLableonora KrasniqiОценок пока нет
- Using NetshДокумент2 страницыUsing NetshMohcin AllaouiОценок пока нет
- 20 Great American Short Stories: Favorite Short Story Collections The Short Story LibraryДокумент10 страниц20 Great American Short Stories: Favorite Short Story Collections The Short Story Librarywileyh100% (1)
- Feb 1 - ScottДокумент17 страницFeb 1 - ScottNyannnОценок пока нет
- Verbal Reasoning TestДокумент3 страницыVerbal Reasoning TesttagawoОценок пока нет
- They Cried MonsterДокумент13 страницThey Cried MonstermassuroОценок пока нет
- Read Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallДокумент1 страницаRead Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallKJRОценок пока нет
- Secant Method - Derivation: A. Bracketing MethodsДокумент5 страницSecant Method - Derivation: A. Bracketing MethodsStephen Dela CruzОценок пока нет
- Character Skills Snapshot Sample ItemsДокумент2 страницыCharacter Skills Snapshot Sample ItemsCharlie BolnickОценок пока нет
- Virtual Verde Release Plan Emails: Email 1Документ4 страницыVirtual Verde Release Plan Emails: Email 1Violet StarОценок пока нет
- The Newton-Leibniz Book Research - Gate - 06!12!2023Документ17 страницThe Newton-Leibniz Book Research - Gate - 06!12!2023Constantine KirichesОценок пока нет
- Mus Culo SkeletalДокумент447 страницMus Culo SkeletalKristine NicoleОценок пока нет
- Types of CostsДокумент9 страницTypes of CostsPrathna AminОценок пока нет
- ESC Cardiomyopathy ClassificationДокумент7 страницESC Cardiomyopathy Classificationvalerius83Оценок пока нет
- SKI Report2008 - 50 2Документ46 страницSKI Report2008 - 50 2nada safitriОценок пока нет
- Tutor InvoiceДокумент13 страницTutor InvoiceAbdullah NHОценок пока нет
- Presentation On HR Department of Mobilink.Документ18 страницPresentation On HR Department of Mobilink.Sadaf YaqoobОценок пока нет
- RH Control - SeracloneДокумент2 страницыRH Control - Seraclonewendys rodriguez, de los santosОценок пока нет