Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Winter2670A 2020 Exam 150421Документ1 страницаWinter2670A 2020 Exam 150421drsneha222 thoratОценок пока нет
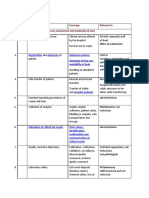
- S.N. Training Topic Coverage Relevant To A. Training Topics Related To Access, Assessment and Continuity of CareДокумент8 страницS.N. Training Topic Coverage Relevant To A. Training Topics Related To Access, Assessment and Continuity of Caredrsneha222 thoratОценок пока нет
- ALS and BLSДокумент17 страницALS and BLSdrsneha222 thoratОценок пока нет
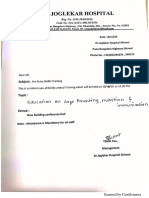
- Traning On Education On Safe Parenting Nutrition and ImmunisationДокумент2 страницыTraning On Education On Safe Parenting Nutrition and Immunisationdrsneha222 thorat100% (2)
- Cataract Manual VISION2020 PDFДокумент80 страницCataract Manual VISION2020 PDFdrsneha222 thoratОценок пока нет
- Nabh Application Eye Care CentreДокумент16 страницNabh Application Eye Care Centredrsneha222 thoratОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Makalah Bahasa Inggris 2Документ7 страницMakalah Bahasa Inggris 2azizah LasimpalaОценок пока нет
- Nurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Документ2 страницыNurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Bianca Nicole Gacad FernandezОценок пока нет
- Osteoporosis: Chandraprakash D. Khedkar Gulab Dattarao KhedkarДокумент7 страницOsteoporosis: Chandraprakash D. Khedkar Gulab Dattarao Khedkardafa bintangОценок пока нет
- Med Chem IV Sem Pre RuhsДокумент1 страницаMed Chem IV Sem Pre Ruhsabhay sharmaОценок пока нет
- Oman Pearsonvue EXAMДокумент7 страницOman Pearsonvue EXAMArun Sabu100% (3)
- 2006 Mesotherapy and Phosphatidylcholine Injections - Historical Clarification and ReviewДокумент16 страниц2006 Mesotherapy and Phosphatidylcholine Injections - Historical Clarification and ReviewDra. Tatiane FariaОценок пока нет
- 8 - Areas of Pharmacy PracticeДокумент30 страниц8 - Areas of Pharmacy PracticeIesoak YagamiОценок пока нет
- Structure and Function of Nervous SystemДокумент58 страницStructure and Function of Nervous SystemFUN FLARE SHADOWОценок пока нет
- Formulation of Multicomponent Cold and Cough SyrupДокумент9 страницFormulation of Multicomponent Cold and Cough SyrupYefii FrisillaОценок пока нет
- Optimization and Formulation of Orodispersible Tablets ofДокумент7 страницOptimization and Formulation of Orodispersible Tablets ofUmar AliОценок пока нет
- Drug StudyДокумент7 страницDrug StudyattydmklcpaОценок пока нет
- Elbaluran Dose Equivelence Drop CardДокумент2 страницыElbaluran Dose Equivelence Drop Cardromany hosnyОценок пока нет
- A Drug Study On EpinephrineДокумент7 страницA Drug Study On EpinephrineMaesy Garcia LorenaОценок пока нет
- Association of Mental Disorders and Psychotropic Medications With Bo - 2022 - BoДокумент6 страницAssociation of Mental Disorders and Psychotropic Medications With Bo - 2022 - BoGeorgiana BunghiuzОценок пока нет
- Chapter 38Документ22 страницыChapter 38Tito, Stephen Gabriel, A.Оценок пока нет
- Cancer Chemotherapy: Acronym of RegimenДокумент13 страницCancer Chemotherapy: Acronym of RegimenVaibhav Bharat100% (1)
- Evaluation of Enzyme Inhibitors in Drug Discovery PDFДокумент2 страницыEvaluation of Enzyme Inhibitors in Drug Discovery PDFMattОценок пока нет
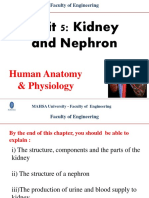
- Unit 5 - Kidney and NephronДокумент30 страницUnit 5 - Kidney and NephronAbdullah MohammedОценок пока нет
- REFERAT Anak TasiaДокумент15 страницREFERAT Anak TasiaAnastasia PasaribuОценок пока нет
- Siddha Marine Drug Palagarai (Cypraea Moneta Linn.) - A ReviewДокумент3 страницыSiddha Marine Drug Palagarai (Cypraea Moneta Linn.) - A ReviewLucasОценок пока нет
- Angel Josabad Alonso-CastroWofSДокумент23 страницыAngel Josabad Alonso-CastroWofSIara PachêcoОценок пока нет
- Macrocytosis - Macrocytic Anemia - UpToDateДокумент36 страницMacrocytosis - Macrocytic Anemia - UpToDateMarvin VillanuevaОценок пока нет
- Hospital Training Report Final 2Документ32 страницыHospital Training Report Final 2Arshad Alam67% (3)
- Chapter 2. WCUДокумент75 страницChapter 2. WCUethiomoney15Оценок пока нет
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesДокумент2 страницыDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleОценок пока нет
- Final Requirement For Dispensing 2Документ2 страницыFinal Requirement For Dispensing 2Blazy InhumangОценок пока нет
- DepakoteДокумент5 страницDepakotejОценок пока нет
- Unverricht-Lundborg Disease A Case Report and LiteДокумент4 страницыUnverricht-Lundborg Disease A Case Report and LiteAndreea CimpoiОценок пока нет
- CV Brown 04232021Документ9 страницCV Brown 04232021api-536548646Оценок пока нет
- Urine TestsДокумент398 страницUrine TestsAliMohamad100% (1)