Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Development of High-Performance Liquid Chromatographic Method For Vitamin D 3 Analysis in Pharmaceutical PreparationДокумент10 страницDevelopment of High-Performance Liquid Chromatographic Method For Vitamin D 3 Analysis in Pharmaceutical PreparationLangit MegaОценок пока нет
- S60 - Morvinandan Diagnostic Centre LLP: Patientreportscsuperpanel - Urine - Examination - SC (Version: 6)Документ10 страницS60 - Morvinandan Diagnostic Centre LLP: Patientreportscsuperpanel - Urine - Examination - SC (Version: 6)Sarah ZiaОценок пока нет
- Unit 2 Vitamins - Essence of HealthДокумент7 страницUnit 2 Vitamins - Essence of HealthKhánh AnОценок пока нет
- PRINCIPALS 7.16..2018 PresentationДокумент21 страницаPRINCIPALS 7.16..2018 Presentationstansimpson1122Оценок пока нет
- OTC Exam 2 Study GuideДокумент32 страницыOTC Exam 2 Study GuideDave WinОценок пока нет
- Jurnal Nutrient of Diet AdolescentДокумент8 страницJurnal Nutrient of Diet AdolescentAnda WarisyaОценок пока нет
- NDT Lec Vitamins and MineralsДокумент18 страницNDT Lec Vitamins and MineralsCrystal MaidenОценок пока нет
- 02 High Blood PressureДокумент8 страниц02 High Blood PressureWalterОценок пока нет
- Nutrients 12 00491Документ30 страницNutrients 12 00491Chon ChiОценок пока нет
- Vitamin A: Sweet Potatoes 28,000 International UnitsДокумент14 страницVitamin A: Sweet Potatoes 28,000 International UnitsTina Avergonzado AmbaОценок пока нет
- TEST BANK Krause's Food & The Nutrition Care Process 13th Edition by L. Kathleen Mahan Janice L Raymond Sylvia Escott StumpДокумент27 страницTEST BANK Krause's Food & The Nutrition Care Process 13th Edition by L. Kathleen Mahan Janice L Raymond Sylvia Escott StumpKieran100% (1)
- Annotated BibliographyДокумент10 страницAnnotated Bibliographyapi-321506941100% (3)
- Intake of Minerals Trace Elements and Vitamins in Bone and Raw Food Rations in Adult DogsДокумент4 страницыIntake of Minerals Trace Elements and Vitamins in Bone and Raw Food Rations in Adult DogsKarl MedinaОценок пока нет
- Bone-Forming Ability of 24r 25-DihydroxyДокумент8 страницBone-Forming Ability of 24r 25-DihydroxyRodrigo ZúñigaОценок пока нет
- Vitamin D Status in Shekhan College StudentsДокумент40 страницVitamin D Status in Shekhan College Studentssirwan ahmadОценок пока нет
- Vitamin DДокумент254 страницыVitamin DAlexi Chávez Echevarría100% (4)
- Vitamins & Minerals: Grade 10Документ55 страницVitamins & Minerals: Grade 10Kayla PyneОценок пока нет
- VMD 512 Zoo/wild Animal Breeding, Nutrition, Management and Health CareДокумент20 страницVMD 512 Zoo/wild Animal Breeding, Nutrition, Management and Health Caresudheer babu arumbaka100% (4)
- MSC - Nursing - Question 2019Документ21 страницаMSC - Nursing - Question 2019Iram AnjumОценок пока нет
- BXXXXX Fall Prevention March 2011Документ20 страницBXXXXX Fall Prevention March 2011Loong Mo MaiОценок пока нет
- 15 PharmacologyДокумент15 страниц15 PharmacologySpy HanОценок пока нет
- The Impact of Vegan Diet On Health and Growth of Children and Adolescents - Literature ReviewДокумент81 страницаThe Impact of Vegan Diet On Health and Growth of Children and Adolescents - Literature ReviewAlexandraОценок пока нет
- Diet Formulation & Common Feed IngredientsДокумент51 страницаDiet Formulation & Common Feed IngredientsJose DeJesus Bustamante Guerrero100% (2)
- 2 Immunonutrition MastersДокумент54 страницы2 Immunonutrition MastersfadihaniОценок пока нет
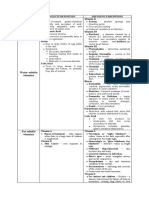
- Water Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin AДокумент3 страницыWater Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ARoshin TejeroОценок пока нет
- Vitamin Part 1 (Compatibility Mode)Документ44 страницыVitamin Part 1 (Compatibility Mode)tamilarasiganasanОценок пока нет
- Fundamentals of HealthCare 50 ItemsДокумент13 страницFundamentals of HealthCare 50 ItemsDefensor Pison Gringgo100% (7)
- Hand Out VITAMINS AND MINERALSДокумент110 страницHand Out VITAMINS AND MINERALSlouie roderos100% (2)
- Shelcal 500Документ5 страницShelcal 500neardrugОценок пока нет
- Responsive Documents - CREW: FTC: Regarding Indoor Tanning Association: 5/15/14 - Batch Two, Part OneДокумент700 страницResponsive Documents - CREW: FTC: Regarding Indoor Tanning Association: 5/15/14 - Batch Two, Part OneCREWОценок пока нет