Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Progress NotesДокумент1 страницаProgress NotesRoxanneGailBigcasGoleroОценок пока нет
- Baicapil™Документ26 страницBaicapil™HarmonyLife100% (6)
- Petcare Power of AttorneyДокумент4 страницыPetcare Power of AttorneyLisaHospetsОценок пока нет
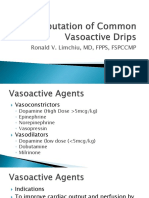
- Computation of Common Vasoactive DripsДокумент23 страницыComputation of Common Vasoactive DripsRoxanneGailBigcasGoleroОценок пока нет
- Intern Logbook FormДокумент2 страницыIntern Logbook FormRoxanneGailBigcasGoleroОценок пока нет
- January: Sun Mon Tue Wed Thu Fri SatДокумент12 страницJanuary: Sun Mon Tue Wed Thu Fri SatRoxanneGailBigcasGoleroОценок пока нет
- Review On Covid-2Документ51 страницаReview On Covid-2RoxanneGailBigcasGoleroОценок пока нет
- Medical Practitioner: Please Do Not DelayДокумент2 страницыMedical Practitioner: Please Do Not DelayRoxanneGailBigcasGoleroОценок пока нет
- Who Pneu Im Pgi ProtocolДокумент2 страницыWho Pneu Im Pgi ProtocolRoxanneGailBigcasGoleroОценок пока нет
- CAP PathophysioДокумент11 страницCAP PathophysioRoxanneGailBigcasGoleroОценок пока нет
- Daily Call Report: Bulacao, Talisay City CebuДокумент1 страницаDaily Call Report: Bulacao, Talisay City CebuRoxanneGailBigcasGoleroОценок пока нет
- Authorization Letter To Pull Out VehicleДокумент1 страницаAuthorization Letter To Pull Out VehicleRoxanneGailBigcasGolero0% (1)
- Authorization Letter To Pull Out VehicleДокумент1 страницаAuthorization Letter To Pull Out VehicleRoxanneGailBigcasGolero0% (1)
- Risk Management PlanДокумент2 страницыRisk Management PlanRoxanneGailBigcasGoleroОценок пока нет
- Family Health Profile (Añonuevo Family) : Purok 2, Brgy. Buyoan, Legazpi CityДокумент11 страницFamily Health Profile (Añonuevo Family) : Purok 2, Brgy. Buyoan, Legazpi CityRoxanneGailBigcasGoleroОценок пока нет
- Order Year Manner OF Delivery AOG Gender Weight ComplicationsДокумент3 страницыOrder Year Manner OF Delivery AOG Gender Weight ComplicationsRoxanneGailBigcasGoleroОценок пока нет
- Republic of The PhilippinesДокумент5 страницRepublic of The PhilippinesRoxanneGailBigcasGoleroОценок пока нет
- (11anh1) Practice Test 3Документ5 страниц(11anh1) Practice Test 3nhuОценок пока нет
- A Drug Study On: Furosemide TabletДокумент7 страницA Drug Study On: Furosemide TabletRaijenne VersolaОценок пока нет
- Practice Guidelines For Obstetric Anesthesia An Updated Report by The American Society of Anesthesiologists Task Force On Obstetric AnesthesiaДокумент14 страницPractice Guidelines For Obstetric Anesthesia An Updated Report by The American Society of Anesthesiologists Task Force On Obstetric AnesthesiaMadalina TalpauОценок пока нет
- Artificial IntelligenceДокумент27 страницArtificial IntelligenceMd HassanОценок пока нет
- SOSCG 6jul2013 v5Документ32 страницыSOSCG 6jul2013 v5Suhazeli Abdullah100% (2)
- Journal Neuropediatri PDFДокумент8 страницJournal Neuropediatri PDFHalimah PramudiyantiОценок пока нет
- Nutrition and MetabolismДокумент179 страницNutrition and MetabolismTuTitОценок пока нет
- Kidney Failure ThesisДокумент8 страницKidney Failure Thesisafcngxbbx100% (3)
- Ulcerative ColitisДокумент30 страницUlcerative ColitisAndika SulistianОценок пока нет
- Evidence-Based Decision Making in Dentistry - Multidisciplinary Management of The Natural DentitionДокумент143 страницыEvidence-Based Decision Making in Dentistry - Multidisciplinary Management of The Natural DentitiontayabakhanОценок пока нет
- Comprehensive Diabetes Checklist Joslin Diabetes CenterДокумент2 страницыComprehensive Diabetes Checklist Joslin Diabetes CenterAbraham DíazОценок пока нет
- Let's Talk Game CardsДокумент4 страницыLet's Talk Game CardssycagurlОценок пока нет
- Treatment of Early Childhood Caries A Case Report 2 1Документ6 страницTreatment of Early Childhood Caries A Case Report 2 1SuciОценок пока нет
- Table of Specification Mapeh 10Документ4 страницыTable of Specification Mapeh 10Melody Anne Dinoso EvangelistaОценок пока нет
- The Human Heart: © 2014 Pearson Education, IncДокумент45 страницThe Human Heart: © 2014 Pearson Education, IncSafee HaiderОценок пока нет
- Dos 773 Csi Plan Study-1Документ7 страницDos 773 Csi Plan Study-1api-504593245Оценок пока нет
- Cases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseДокумент3 страницыCases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseIrma Suriani DarwisОценок пока нет
- Music Has The Power To HealДокумент16 страницMusic Has The Power To HealBalajiОценок пока нет
- Automated CLIA Analyzers-171222 - ITKДокумент14 страницAutomated CLIA Analyzers-171222 - ITKmОценок пока нет
- Ventilation: Kinematics and Kinetics.: Thorax Structure and FunctionДокумент52 страницыVentilation: Kinematics and Kinetics.: Thorax Structure and FunctionAlejandra RomeroОценок пока нет
- Hea LLG: 18 Sign of Dehydration - ThirstДокумент22 страницыHea LLG: 18 Sign of Dehydration - ThirstMhae TabasaОценок пока нет
- Cocaine and HeroinДокумент48 страницCocaine and Heroinzio riaОценок пока нет
- Deep Breathing Relaxation For Decreasing Blood Pressure in People With HypertensionДокумент5 страницDeep Breathing Relaxation For Decreasing Blood Pressure in People With HypertensionFriska HarianjaОценок пока нет
- Newborn Buried Alive:: Transgender'S RevengeДокумент16 страницNewborn Buried Alive:: Transgender'S RevengeAbhishekh GuptaОценок пока нет
- Applications of Deep Learning and Machine Learning in Healthcare Domain - A Literature ReviewДокумент14 страницApplications of Deep Learning and Machine Learning in Healthcare Domain - A Literature ReviewIAEME PublicationОценок пока нет
- Stroke Signs and Symptoms - CDC - GovДокумент2 страницыStroke Signs and Symptoms - CDC - Govjeanne_mbОценок пока нет
- Excretory Products and Their EliminationДокумент9 страницExcretory Products and Their EliminationBiju MylachalОценок пока нет
- Low Risk Labour CareДокумент11 страницLow Risk Labour CareYwagar YwagarОценок пока нет