Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Stat and Prob Q1 M2Документ10 страницStat and Prob Q1 M2Sakusaku100% (1)
- Variables and ValuesДокумент7 страницVariables and ValuesAbdul Manan SaeedОценок пока нет
- Practical Research 2Документ127 страницPractical Research 2Zeru Vill50% (2)
- Lecture 4 Day 3 Stochastic Frontier AnalysisДокумент45 страницLecture 4 Day 3 Stochastic Frontier AnalysisJennifer Lee100% (7)
- BB Day 2 ExamДокумент6 страницBB Day 2 Exammohamed guedichiОценок пока нет
- Comparison of Quantitative and Qualitative Research Traditions: Epistemological, Theoretical, and Methodological DifferencesДокумент16 страницComparison of Quantitative and Qualitative Research Traditions: Epistemological, Theoretical, and Methodological DifferencesRendorn Guerrin100% (1)
- Comparing Biodiversity SpidersДокумент4 страницыComparing Biodiversity Spidersapi-235658421Оценок пока нет
- Answer Any Four Questions. Use Appropriate Software For Analysis and Copy Results Into Microsoft Word With A File Name After Your NameДокумент1 страницаAnswer Any Four Questions. Use Appropriate Software For Analysis and Copy Results Into Microsoft Word With A File Name After Your NameipilakyaaОценок пока нет
- 12 Mar - AssQДокумент3 страницы12 Mar - AssQjigar9161Оценок пока нет
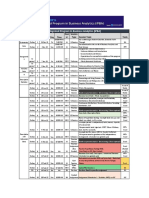
- Integrtaed Program in Business Analytics - Batch 11 ScheduleДокумент4 страницыIntegrtaed Program in Business Analytics - Batch 11 SchedulesОценок пока нет
- Mathematical Modeling Using Linear RegresionДокумент52 страницыMathematical Modeling Using Linear RegresionIrinel IonutОценок пока нет
- Annual Education Statistics 2009Документ165 страницAnnual Education Statistics 2009dochula7745Оценок пока нет
- Assignment 04 ProblemДокумент7 страницAssignment 04 ProblemRAGHAV GABA IPM 2019-24 BatchОценок пока нет
- Golbraikh, Beware of q2Документ8 страницGolbraikh, Beware of q2Muhammad IrmansyahОценок пока нет
- Jmodeltest 0.1.1: (April 2008)Документ23 страницыJmodeltest 0.1.1: (April 2008)เอ็นจอย ไลฟ์Оценок пока нет
- Relationship Between Consumer Characteristics and Impulse Buying Behavior - The Mediating Role of Buying Intention of New Clothing Buyers (#355400) - 367047 PDFДокумент8 страницRelationship Between Consumer Characteristics and Impulse Buying Behavior - The Mediating Role of Buying Intention of New Clothing Buyers (#355400) - 367047 PDFramОценок пока нет
- Post Graduate Diploma in Bio Statistics and Data ManagementДокумент4 страницыPost Graduate Diploma in Bio Statistics and Data ManagementvijaynaroteОценок пока нет
- Maths for ML: Linear Regression to Bayesian LDAДокумент134 страницыMaths for ML: Linear Regression to Bayesian LDADaria GodorozhaОценок пока нет
- Forward Backward ChainingДокумент5 страницForward Backward ChainingAnshika TyagiОценок пока нет
- Grade 7 Week 3 Las 2Документ2 страницыGrade 7 Week 3 Las 2MONHANNAH RAMADEAH LIMBUTUNGANОценок пока нет
- 1 Introduction To Optimum Design PDFДокумент15 страниц1 Introduction To Optimum Design PDFAugusto De La Cruz CamayoОценок пока нет
- SPSSДокумент25 страницSPSSBhawana SharmaОценок пока нет
- SWGDRUG Recommendations Version 8 - FINAL - ForPosting - 092919Документ83 страницыSWGDRUG Recommendations Version 8 - FINAL - ForPosting - 092919Diego Rissi CarvalhosaОценок пока нет
- IUP 18 Assign1Документ3 страницыIUP 18 Assign1swethaОценок пока нет
- Hydrology PaperДокумент26 страницHydrology Papersaiba0% (1)
- Syllabus RegressionДокумент2 страницыSyllabus RegressionShashank BhaskerОценок пока нет
- Problem Set 8Документ3 страницыProblem Set 8JonahJunior0% (1)
- Mathematics 8 Analytic Rubric - Statistics and Probability Criteria Excellent 4 Very Good 3 Good 2 Needs Improvement 1Документ2 страницыMathematics 8 Analytic Rubric - Statistics and Probability Criteria Excellent 4 Very Good 3 Good 2 Needs Improvement 1Melissa LouiseОценок пока нет
- Improve Iso 14001Документ12 страницImprove Iso 14001Trang Hà VũОценок пока нет
- IJRAR19W1527Документ15 страницIJRAR19W1527Raghu YogОценок пока нет