Вам также может понравиться
- Forklift Safety Policy and ProcedureДокумент3 страницыForklift Safety Policy and ProcedureChristian Auditor Rivera100% (1)
- Risk Assessments For ACTIVITY BASEDДокумент4 страницыRisk Assessments For ACTIVITY BASEDhello3232Оценок пока нет
- Monthly HSE report summaryДокумент5 страницMonthly HSE report summaryNiraОценок пока нет
- Safety Management MidtermДокумент23 страницыSafety Management MidtermKent Edve Neil Rabe100% (1)
- Daily Vehicle Inspection Checklist 11 09 WfeelefyoppyДокумент1 страницаDaily Vehicle Inspection Checklist 11 09 Wfeelefyoppyrajesh kumarОценок пока нет
- Job Safety Analysis: Calalang Residence J. Fajardo St. Sampaloc ManillaДокумент4 страницыJob Safety Analysis: Calalang Residence J. Fajardo St. Sampaloc ManillaJoey Stanley GuzmanОценок пока нет
- Ladder Inspection ChecklistДокумент1 страницаLadder Inspection ChecklistArshad MahmoodОценок пока нет
- Toolbox Talks Pneumatic Tools EnglishДокумент1 страницаToolbox Talks Pneumatic Tools EnglishebbasinghОценок пока нет
- 13.2.4 RA SWP For Cable Installation Glanding Terminating Testing To Site Cabins at DCLДокумент13 страниц13.2.4 RA SWP For Cable Installation Glanding Terminating Testing To Site Cabins at DCLMARIAN100% (1)
- JHA Example Installation of Underfloor Plumbing and DrainsДокумент15 страницJHA Example Installation of Underfloor Plumbing and DrainsShamel Jen FacundoОценок пока нет
- Welding Checklist 9195Документ3 страницыWelding Checklist 9195Michael PenaОценок пока нет
- Office Risk AssessmentДокумент4 страницыOffice Risk AssessmentRameeSahiba100% (1)
- Tool Box Talk 11 Working On RoofsДокумент1 страницаTool Box Talk 11 Working On RoofsRomanuSОценок пока нет
- Scaffolding-Fixed and Mobile: Safety Operating ProceduresДокумент1 страницаScaffolding-Fixed and Mobile: Safety Operating Proceduresmohammed muzammilОценок пока нет
- Internal OHS Audit Methodology PDFДокумент8 страницInternal OHS Audit Methodology PDFPaul MaposaОценок пока нет
- Accident/Incident/Near-miss InvestigationДокумент6 страницAccident/Incident/Near-miss InvestigationJakir Hossain TonyОценок пока нет
- Heat Stress ProcedureДокумент13 страницHeat Stress ProcedureKneekEy CastleОценок пока нет
- Manual Handling Safe Work InstructionДокумент3 страницыManual Handling Safe Work InstructionUvini IndurangaОценок пока нет
- Office Risk AssessmentДокумент3 страницыOffice Risk AssessmentFrenchieL100% (1)
- Toolbox Talk - Mounting and Dismounting EquipmentДокумент1 страницаToolbox Talk - Mounting and Dismounting Equipmentsl1828Оценок пока нет
- Fall Protection Risk AssessmentДокумент3 страницыFall Protection Risk Assessmentsimone0% (1)
- JSA ScaffoldingДокумент2 страницыJSA Scaffoldingmyco samОценок пока нет
- Excavation and Trenching Safety PlanДокумент21 страницаExcavation and Trenching Safety Planleonardo Garais100% (1)
- Construction Assessment Checklist: Green TagДокумент2 страницыConstruction Assessment Checklist: Green TagRyan GillespieОценок пока нет
- A002 C NightclubДокумент6 страницA002 C NightclubBlas de LezoОценок пока нет
- Very Very Good Risk Assessment EnvironmentДокумент8 страницVery Very Good Risk Assessment EnvironmentSalley Bukhari100% (1)
- Risk Assessment For Partition MarkingДокумент5 страницRisk Assessment For Partition Markingkhalid14Оценок пока нет
- Fire Extingisher Inspection ProcedureДокумент2 страницыFire Extingisher Inspection ProcedurewaheedОценок пока нет
- Grinding Equipment Risk AssessmentДокумент3 страницыGrinding Equipment Risk Assessmentdroffilcz270% (1)
- Risk Assesment For Demolition of Factory Buildings at 14 Tuas Ave 1Документ4 страницыRisk Assesment For Demolition of Factory Buildings at 14 Tuas Ave 1Yam Balaoing100% (1)
- Safety Incident ProcedureДокумент15 страницSafety Incident Proceduresivaguruaks100% (1)
- Saf 113 A Daily She Inspection Report 1Документ4 страницыSaf 113 A Daily She Inspection Report 1saravana3kumar3ravic100% (1)
- Tool Box TalksДокумент82 страницыTool Box TalksMuhammad Asif MehmudОценок пока нет
- WAH Scaffold Inspection Sheet PDFДокумент1 страницаWAH Scaffold Inspection Sheet PDFMKhairulMDОценок пока нет
- Working Heights Risk Assessment TemplateДокумент8 страницWorking Heights Risk Assessment TemplatePanchdev KumarОценок пока нет
- Hot Work PermitДокумент2 страницыHot Work PermitAndiWSutomoОценок пока нет
- Incident & Accident ReportДокумент7 страницIncident & Accident ReportleganzaОценок пока нет
- Ppe Issue List For ContractorsДокумент2 страницыPpe Issue List For ContractorsMartellR100% (1)
- Safety Committee Meeting Minutes TemplateДокумент3 страницыSafety Committee Meeting Minutes TemplateKashémОценок пока нет
- Job Safety Analysis: JSA Reference #: DateДокумент3 страницыJob Safety Analysis: JSA Reference #: DateLi QiОценок пока нет
- Monthly Site Safety Audit ReportДокумент3 страницыMonthly Site Safety Audit Reporttajshah283100% (1)
- Title: Hot Work Procedure: Occupational Health and Safety Act 2004 Occupational Health and Safety Regulations 2007Документ5 страницTitle: Hot Work Procedure: Occupational Health and Safety Act 2004 Occupational Health and Safety Regulations 2007Adeyinka MichealОценок пока нет
- 1 Control of HazardousДокумент5 страниц1 Control of HazardousVinz Hexon BalangueОценок пока нет
- Baseline Risk AssessmentДокумент6 страницBaseline Risk AssessmentPHUMZILEОценок пока нет
- Accident Reporting PolicyДокумент2 страницыAccident Reporting PolicybmkallarackalОценок пока нет
- 02 General Aspect Impact StudyДокумент1 страница02 General Aspect Impact StudymakdelОценок пока нет
- Fall Protection Risk AssessmentДокумент3 страницыFall Protection Risk AssessmentsimoneОценок пока нет
- Safe Work ProcedureДокумент2 страницыSafe Work ProcedureSuco IdeunkОценок пока нет
- Incident Report: Proj. N. Unit Document Code Serial NДокумент1 страницаIncident Report: Proj. N. Unit Document Code Serial NSyed Ali HassanОценок пока нет
- ISBN Sample OHS Action Plan For Community Services Sector 2007 01 PDFДокумент5 страницISBN Sample OHS Action Plan For Community Services Sector 2007 01 PDFpurva02Оценок пока нет
- Risk Assement RegisterДокумент10 страницRisk Assement RegisterAnonymous OmLE7heOОценок пока нет
- Toolbox TalksДокумент255 страницToolbox TalksisaacbombayОценок пока нет
- Lockout Tagout TRNG GuideДокумент7 страницLockout Tagout TRNG GuideSyed Mujtaba Ali Bukhari100% (1)
- Safety InductionДокумент52 страницыSafety InductionBenard OdhiamboОценок пока нет
- Ks3 Science 2008 Level 5 7 Paper 1Документ28 страницKs3 Science 2008 Level 5 7 Paper 1Saima Usman - 41700/TCHR/MGBОценок пока нет
- Yanmar America publication listing for engine parts, service, and operation manualsДокумент602 страницыYanmar America publication listing for engine parts, service, and operation manualsEnrique Murgia50% (2)
- Advantages and Disadvantages of The DronesДокумент43 страницыAdvantages and Disadvantages of The DronesVysual ScapeОценок пока нет
- Emerson Park Master Plan 2015 DraftДокумент93 страницыEmerson Park Master Plan 2015 DraftRyan DeffenbaughОценок пока нет
- Philips DVD Player SpecificationsДокумент2 страницыPhilips DVD Player Specificationsbhau_20Оценок пока нет
- Doe v. Myspace, Inc. Et Al - Document No. 37Документ2 страницыDoe v. Myspace, Inc. Et Al - Document No. 37Justia.comОценок пока нет
- Machine Spindle Noses: 6 Bison - Bial S. AДокумент2 страницыMachine Spindle Noses: 6 Bison - Bial S. AshanehatfieldОценок пока нет
- Insize Catalogue 2183,2392Документ1 страницаInsize Catalogue 2183,2392calidadcdokepОценок пока нет
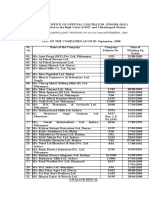
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Документ4 страницыStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20Оценок пока нет
- Land Measurement in PunjabДокумент3 страницыLand Measurement in PunjabJunaid Iqbal33% (3)
- Huawei WCDMA Primary Scrambling Code PlanningДокумент22 страницыHuawei WCDMA Primary Scrambling Code PlanningZeljko Vrankovic90% (31)
- Lecture 1 Family PlanningДокумент84 страницыLecture 1 Family PlanningAlfie Adam Ramillano100% (4)
- Unit 1 - Introduction To BankingДокумент17 страницUnit 1 - Introduction To Bankingc08Оценок пока нет
- EE290 Practice 3Документ4 страницыEE290 Practice 3olgaОценок пока нет
- SQL Server 2008 Failover ClusteringДокумент176 страницSQL Server 2008 Failover ClusteringbiplobusaОценок пока нет
- Guidelines Tax Related DeclarationsДокумент16 страницGuidelines Tax Related DeclarationsRaghul MuthuОценок пока нет
- JSA - 0026 Chipping & Granite cutting and lying Work At PB-19Документ2 страницыJSA - 0026 Chipping & Granite cutting and lying Work At PB-19Koneti JanardhanaraoОценок пока нет
- Binomial ExpansionДокумент13 страницBinomial Expansion3616609404eОценок пока нет
- Impolitic Art Sparks Debate Over Societal ValuesДокумент10 страницImpolitic Art Sparks Debate Over Societal ValuesCarine KmrОценок пока нет
- Hawk Technology Systems v. NCLДокумент6 страницHawk Technology Systems v. NCLPriorSmartОценок пока нет
- Modified Release Drug ProductsДокумент58 страницModified Release Drug Productsmailtorubal2573100% (2)
- Single-Phase Induction Generators PDFДокумент11 страницSingle-Phase Induction Generators PDFalokinxx100% (1)
- IntroductionДокумент34 страницыIntroductionmarranОценок пока нет
- PW CДокумент4 страницыPW CAnonymous DduElf20OОценок пока нет
- Determination of Vitamin C in FoodsДокумент11 страницDetermination of Vitamin C in FoodsDalal Shab JakhodiyaОценок пока нет
- Numerical Methods: Jeffrey R. ChasnovДокумент60 страницNumerical Methods: Jeffrey R. Chasnov2120 sanika GaikwadОценок пока нет
- Electrosteel Castings Limited (ECL) - Technology That CaresДокумент4 страницыElectrosteel Castings Limited (ECL) - Technology That CaresUjjawal PrakashОценок пока нет
- Instagram Dan Buli Siber Dalam Kalangan Remaja Di Malaysia: Jasmyn Tan YuxuanДокумент13 страницInstagram Dan Buli Siber Dalam Kalangan Remaja Di Malaysia: Jasmyn Tan YuxuanXiu Jiuan SimОценок пока нет
- Irctc Tour May 2023Документ6 страницIrctc Tour May 2023Mysa ChakrapaniОценок пока нет
- Cinema 4D ShortcutsДокумент8 страницCinema 4D ShortcutsAnonymous 0lRguGОценок пока нет