Вам также может понравиться
- PPS CPG UtiДокумент8 страницPPS CPG UtiPaula QuiñonesОценок пока нет
- CPM7th TB in Infancy and ChildhoodДокумент41 страницаCPM7th TB in Infancy and ChildhoodJackyОценок пока нет
- PM PFC MatrixДокумент4 страницыPM PFC MatrixFamed residentsОценок пока нет
- Papp Perspective: Philippine Academy of Pediatric Pulmonologists, IncДокумент54 страницыPapp Perspective: Philippine Academy of Pediatric Pulmonologists, IncMarko Parungo100% (1)
- CPG Uti PDFДокумент7 страницCPG Uti PDFhellokathyyyyyy100% (1)
- REVALIDA EXAM 200 Answers With RationaleДокумент17 страницREVALIDA EXAM 200 Answers With Rationalexaileenx100% (1)
- ROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsДокумент2 страницыROO M General Data Admitt Ing DX Worki NG DX Laboratory Frichmond MedicationsnicewanОценок пока нет
- Pathophysiology of Dengue FeverДокумент1 страницаPathophysiology of Dengue FeverApple Mae100% (1)
- Revalida QuestionsДокумент9 страницRevalida QuestionserwinsanОценок пока нет
- Neonatal Pneumonia Case StudyДокумент2 страницыNeonatal Pneumonia Case StudyAngel Villamor0% (1)
- Dengue PathophysiologyДокумент1 страницаDengue PathophysiologyRafael Miguel Alon Protacio50% (2)
- Neonatal SepsisДокумент87 страницNeonatal Sepsisyhanne100% (129)
- Oral Revalida 2019Документ28 страницOral Revalida 2019April Cabarlo100% (6)
- Topnotch Microbiology Supertable - by DR - Cocoy Calderon, Jaffar Pineda, Troy SoberanoДокумент3 страницыTopnotch Microbiology Supertable - by DR - Cocoy Calderon, Jaffar Pineda, Troy SoberanoJohn Christopher Luces100% (1)
- Febrile SeizuresДокумент5 страницFebrile SeizuresJulmajir Salipmugdar100% (1)
- Case Study Neonatal SepsisДокумент21 страницаCase Study Neonatal SepsisLenjun0% (1)
- Philippine Pediatric Society, IncДокумент19 страницPhilippine Pediatric Society, IncAsmphLibrary OrtigasОценок пока нет
- PPS Core PediatricsДокумент53 страницыPPS Core PediatricsDenise Castro100% (3)
- 09 Pediatrics PLE 2019 RatioДокумент66 страниц09 Pediatrics PLE 2019 RatioMei Bejerano - Roldan100% (1)
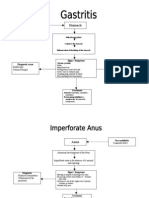
- Gastro PathophysiologyДокумент4 страницыGastro PathophysiologyPaul JoloОценок пока нет
- Luminare PGI Primer PDFДокумент62 страницыLuminare PGI Primer PDFChristine Evan HoОценок пока нет
- Preventive Pediatrics 2016Документ48 страницPreventive Pediatrics 2016riz04_fortitudessa5178100% (9)
- CPG On Acute GastroenteritisДокумент24 страницыCPG On Acute GastroenteritisAbegail Fermanejo-Generao100% (1)
- Neonatal Sepsis PathophysiologyДокумент4 страницыNeonatal Sepsis PathophysiologyAlex Marie100% (4)
- Pediatric Clinical H&PДокумент7 страницPediatric Clinical H&PJay Vee100% (1)
- Reflection Family MedicineДокумент3 страницыReflection Family MedicineStanley SekwenaОценок пока нет
- Dengue Fever Discharge PlanДокумент9 страницDengue Fever Discharge PlanTrisha Faye OrtegaОценок пока нет
- Pa Tho Physiology of DengueДокумент1 страницаPa Tho Physiology of Denguesinister17100% (1)
- Topnotch Pediatrics For MoonlightersДокумент323 страницыTopnotch Pediatrics For Moonlightersmefav7778520100% (1)
- Pedia Idiot Notes 1Документ12 страницPedia Idiot Notes 1David JonesОценок пока нет
- Patient-Centered, Family Focused, Community Oriented Care MatrixДокумент13 страницPatient-Centered, Family Focused, Community Oriented Care MatrixJesse MonsalveОценок пока нет
- September 2021 PleДокумент20 страницSeptember 2021 PleGian PagadduОценок пока нет
- Screem-Res Description 1Документ4 страницыScreem-Res Description 1Jeanne Marie Vales100% (2)
- PPS Policies RevisedДокумент27 страницPPS Policies RevisedAnneCanapi100% (1)
- CPG On CsomДокумент8 страницCPG On CsomRobert Ross DulayОценок пока нет
- Viral Exanthems PDFДокумент67 страницViral Exanthems PDFChristopher AdhisasmitaОценок пока нет
- Preventive Medicine PLE ReviewerДокумент4 страницыPreventive Medicine PLE ReviewerReinhard Ivan MansibangОценок пока нет
- Case - LeptospirosisДокумент39 страницCase - LeptospirosisKimm Delos ReyesОценок пока нет
- Case Presentation GastroenteritisДокумент58 страницCase Presentation GastroenteritisShereen Manabilang100% (3)
- 11 Topnotch Pediatrics SuperExam PDFДокумент97 страниц11 Topnotch Pediatrics SuperExam PDFDre Valdez100% (4)
- Course in The Wards FormatДокумент2 страницыCourse in The Wards FormatJade MonrealОценок пока нет
- OB Nursing Care PlanДокумент3 страницыOB Nursing Care PlanLiza Marie Cayetano AdarneОценок пока нет
- DengueДокумент4 страницыDengueKathleen DimacaliОценок пока нет
- Final Coaching - Obgyne 2022Документ7 страницFinal Coaching - Obgyne 2022Jhon PauloОценок пока нет
- Chronic Suppurative Otitis Media in AdultsДокумент10 страницChronic Suppurative Otitis Media in AdultsRstadam TagalogОценок пока нет
- DEngue FlowchartДокумент2 страницыDEngue FlowchartJelly Cruz100% (3)
- Pathophysiology Dengue 2Документ4 страницыPathophysiology Dengue 2KatherineОценок пока нет
- 8 Neonatal Sepsis 2019Документ45 страниц8 Neonatal Sepsis 2019Yan Zhen YuanОценок пока нет
- Acute Gastroenteritis (Meta)Документ77 страницAcute Gastroenteritis (Meta)Al-nazer Azer AlОценок пока нет
- Dengue PoathoДокумент6 страницDengue PoathoCleobebs Agustin100% (1)
- Wilm's Tumor Pa Tho PhysiologyДокумент1 страницаWilm's Tumor Pa Tho Physiologya_yeLОценок пока нет
- 1.who Shall Be Considered As Having Community-Acquired Pneumonia?Документ6 страниц1.who Shall Be Considered As Having Community-Acquired Pneumonia?Kristine Jade OdtujanОценок пока нет
- Pathophysiology of SLEДокумент16 страницPathophysiology of SLESeff CausapinОценок пока нет
- Summary Proceedings From The Neurology Group On Neonatal SeizuresДокумент7 страницSummary Proceedings From The Neurology Group On Neonatal SeizuresTran Trang AnhОценок пока нет
- Encefalopatia Neonatal PDFДокумент13 страницEncefalopatia Neonatal PDFVanessa RomeroОценок пока нет
- Guidelines VertigoДокумент16 страницGuidelines VertigoririnОценок пока нет
- Estatus Epileptico de Nuevo Inicio (NORSE)Документ8 страницEstatus Epileptico de Nuevo Inicio (NORSE)juanutОценок пока нет
- Epilepsy Syndromes inДокумент24 страницыEpilepsy Syndromes inEdwin AlvarezОценок пока нет
- Approach To Refractory Childhood SeizuresДокумент10 страницApproach To Refractory Childhood SeizureskholisahnasutionОценок пока нет
- Management and Investigation of Neonatal Encephalopathy: 2017 UpdateДокумент13 страницManagement and Investigation of Neonatal Encephalopathy: 2017 Updatenuge putriОценок пока нет
- Spinal Anesthesia: Ji Mandal Ji Solonio Ji Tumanan Ji TuveraДокумент32 страницыSpinal Anesthesia: Ji Mandal Ji Solonio Ji Tumanan Ji TuveraGehlatin TumananОценок пока нет
- Pathophysiology of Rheumatic FeverДокумент3 страницыPathophysiology of Rheumatic FeverGehlatin Tumanan100% (2)
- January 2021: SUN MON TUE WED THU FRI SATДокумент12 страницJanuary 2021: SUN MON TUE WED THU FRI SATGehlatin TumananОценок пока нет
- Naturukan Ka Ba NG Anesthesia? Bakit Di Mo Maramdamang Mahal Kita?Документ2 страницыNaturukan Ka Ba NG Anesthesia? Bakit Di Mo Maramdamang Mahal Kita?Gehlatin TumananОценок пока нет
- Dengue DOHДокумент16 страницDengue DOHGehlatin Tumanan100% (1)
- Partying Smoking Joining of Fraternity Substance Abuse: Desire To Be HappyДокумент1 страницаPartying Smoking Joining of Fraternity Substance Abuse: Desire To Be HappyGehlatin TumananОценок пока нет
- General Adaptation SyndromeДокумент4 страницыGeneral Adaptation SyndromeGehlatin Tumanan100% (1)
- Artificial AirwaysДокумент68 страницArtificial AirwaysGehlatin TumananОценок пока нет
- Respiratory Cytology: DR Mohammed Shahin, JR (Academic), Dept of Pathology & Lab Medicine, AIIMS BhubaneswarДокумент62 страницыRespiratory Cytology: DR Mohammed Shahin, JR (Academic), Dept of Pathology & Lab Medicine, AIIMS BhubaneswarShruthi N.RОценок пока нет
- Prenatal and Postnatal Care A Woman Centered Approach 2nd EditionДокумент61 страницаPrenatal and Postnatal Care A Woman Centered Approach 2nd Editionmarion.wade943Оценок пока нет
- 8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013Документ13 страниц8 Pseudocyst of Pinna and Its Treatment With Surgical Deroofing - An Experience at Tertiary Hospitals 2013solikin ikinОценок пока нет
- Lesson 14 NDT Report EditedДокумент30 страницLesson 14 NDT Report Editedmagicrjay26Оценок пока нет
- Literature Review Example AmaДокумент6 страницLiterature Review Example Amatkpmzasif100% (1)
- Viral Skin Infections: Verrucae ValgarusДокумент14 страницViral Skin Infections: Verrucae Valgarusمسلم هاشم منافОценок пока нет
- Pharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraДокумент39 страницPharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraKim Nicole Villaflores0% (1)
- What Is Atrial FibrillationДокумент3 страницыWhat Is Atrial FibrillationMoni ShafiqОценок пока нет
- Total Hip Replacement Recovery & Surgery Complications - Dr. Vinil ShindeДокумент2 страницыTotal Hip Replacement Recovery & Surgery Complications - Dr. Vinil ShindeDr VInil ShindeОценок пока нет
- AEFIДокумент33 страницыAEFIAnuradha JaiswalОценок пока нет
- Chellah Final Research (2) EditedДокумент56 страницChellah Final Research (2) EditedCredible Technology ComplexОценок пока нет
- Armitage 2013 ReviewДокумент17 страницArmitage 2013 ReviewMarcoОценок пока нет
- RumenotomyДокумент1 страницаRumenotomymake it make senseОценок пока нет
- MALNUTRITIONДокумент23 страницыMALNUTRITIONPrincess Alane MorenoОценок пока нет
- Medical Evaluation of Adverse Events in Pharmacovigilance Global Perspective of PharmacovigilanceДокумент6 страницMedical Evaluation of Adverse Events in Pharmacovigilance Global Perspective of PharmacovigilanceAdalbert P ShaОценок пока нет
- Development and Content Validity of A Website ForДокумент7 страницDevelopment and Content Validity of A Website Forrickelme.businessОценок пока нет
- Mini-Review: Neonatal PolycythaemiaДокумент3 страницыMini-Review: Neonatal PolycythaemiaElizabeth HendersonОценок пока нет
- ICD-9-CM To ICD-10 Common Codes For Cardiovascular Disease: A Quick Reference For Quest Diagnostics ClientsДокумент1 страницаICD-9-CM To ICD-10 Common Codes For Cardiovascular Disease: A Quick Reference For Quest Diagnostics Clientssyaiful rinantoОценок пока нет
- Clinical PsyДокумент12 страницClinical PsyAsfatin AmranОценок пока нет
- Hepatocellular Carcinoma and Other Hepatic MassesДокумент59 страницHepatocellular Carcinoma and Other Hepatic MassesIsaac MwangiОценок пока нет
- EAU Guidelines On Male Sexual Dysfunction 2019Документ96 страницEAU Guidelines On Male Sexual Dysfunction 2019Muti IlmarifaОценок пока нет
- BZYET 143 EnglishДокумент4 страницыBZYET 143 EnglishSangita PaulОценок пока нет
- Pathophysiology of Pressure UlcersДокумент1 страницаPathophysiology of Pressure UlcersSTORAGE FILEОценок пока нет
- Mitochondrial Disorders A Review of Anesthetic ConsiderationsДокумент10 страницMitochondrial Disorders A Review of Anesthetic ConsiderationsSanaОценок пока нет
- MainДокумент12 страницMainmarco enriquezОценок пока нет
- Garcia, Poligrates: Sinus & FistulaДокумент2 страницыGarcia, Poligrates: Sinus & FistulaPaulo GarciaОценок пока нет
- Herbal Medicine For EveryoneДокумент63 страницыHerbal Medicine For EveryoneMaratus Solehah100% (2)
- Artificial Nutrition and Hydration at The End of LifeДокумент40 страницArtificial Nutrition and Hydration at The End of LifeRazaCreciaLastrillaMenesesОценок пока нет
- Infectious Disease of The HeartДокумент3 страницыInfectious Disease of The HeartClaire GidoОценок пока нет
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildОт EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildРейтинг: 3.5 из 5 звезд3.5/5 (9)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionОт EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionРейтинг: 4.5 из 5 звезд4.5/5 (2)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsОт EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsОценок пока нет
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsОт EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousОт EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousРейтинг: 5 из 5 звезд5/5 (22)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductОт EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductРейтинг: 5 из 5 звезд5/5 (31)
- Guts: The Endless Follies and Tiny Triumphs of a Giant DisasterОт EverandGuts: The Endless Follies and Tiny Triumphs of a Giant DisasterРейтинг: 4 из 5 звезд4/5 (99)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryОт EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryОценок пока нет
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerОт EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerРейтинг: 5 из 5 звезд5/5 (8)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryОт EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryРейтинг: 5 из 5 звезд5/5 (47)
- 12 Step Spirituality: Every Person’s Guide to Taking the Twelve StepsОт Everand12 Step Spirituality: Every Person’s Guide to Taking the Twelve StepsРейтинг: 5 из 5 звезд5/5 (17)
- The Easy Way to Stop Gambling: Take Control of Your LifeОт EverandThe Easy Way to Stop Gambling: Take Control of Your LifeРейтинг: 4 из 5 звезд4/5 (197)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.От EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Рейтинг: 4 из 5 звезд4/5 (7)
- Canary in the Coal Mine: A Forgotten Rural Community, a Hidden Epidemic, and a Lone Doctor Battling for the Life, Health, and Soul of the PeopleОт EverandCanary in the Coal Mine: A Forgotten Rural Community, a Hidden Epidemic, and a Lone Doctor Battling for the Life, Health, and Soul of the PeopleРейтинг: 4 из 5 звезд4/5 (3)
- Psilocybin Mushrooms: A Practical Guide to the Types and Magic Effects of Psychedelic MushroomsОт EverandPsilocybin Mushrooms: A Practical Guide to the Types and Magic Effects of Psychedelic MushroomsРейтинг: 4 из 5 звезд4/5 (14)
- Easyway Express: Stop Smoking and Quit E-CigarettesОт EverandEasyway Express: Stop Smoking and Quit E-CigarettesРейтинг: 5 из 5 звезд5/5 (15)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingОт EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingРейтинг: 5 из 5 звезд5/5 (10)
- Blood Orange Night: My Journey to the Edge of MadnessОт EverandBlood Orange Night: My Journey to the Edge of MadnessРейтинг: 4 из 5 звезд4/5 (42)
- Addiction and Grace: Love and Spirituality in the Healing of AddictionsОт EverandAddiction and Grace: Love and Spirituality in the Healing of AddictionsРейтинг: 4.5 из 5 звезд4.5/5 (11)
- Living Sober: Practical methods alcoholics have used for living without drinkingОт EverandLiving Sober: Practical methods alcoholics have used for living without drinkingРейтинг: 4 из 5 звезд4/5 (50)
- You Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugОт EverandYou Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugОценок пока нет
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingОт EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingРейтинг: 5 из 5 звезд5/5 (11)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionОт EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionРейтинг: 5 из 5 звезд5/5 (63)