Вам также может понравиться
- Plete ToolkitДокумент54 страницыPlete ToolkitPsydocОценок пока нет
- The ADHD Workbook for Parents: A Guide for Parents of Children Ages 212 with Attention-Deficit/Hyperactivity DisorderОт EverandThe ADHD Workbook for Parents: A Guide for Parents of Children Ages 212 with Attention-Deficit/Hyperactivity DisorderРейтинг: 5 из 5 звезд5/5 (4)
- Adhd PsychoeducationДокумент4 страницыAdhd Psychoeducationapi-487140745100% (1)
- A Beginner's Guide on Parenting Kids with ADHD: Navigating the ADHD Journey: A New Parent's Comprehensive and Practical Handbook to Parenting Kids with ADHDОт EverandA Beginner's Guide on Parenting Kids with ADHD: Navigating the ADHD Journey: A New Parent's Comprehensive and Practical Handbook to Parenting Kids with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- ADHD Parent Skills Training ManualДокумент85 страницADHD Parent Skills Training ManualLalita Marathe100% (1)
- Clinicians Guide To AutismДокумент20 страницClinicians Guide To AutismNadia Desanti RachmatikaОценок пока нет
- The Adult ADHD Handbook for Patients, Family & FriendsОт EverandThe Adult ADHD Handbook for Patients, Family & FriendsРейтинг: 3 из 5 звезд3/5 (1)
- Adhdconnors SelfДокумент1 страницаAdhdconnors Selfapi-252732354Оценок пока нет
- SNAP-IV-C Rating Scale # 6160Документ1 страницаSNAP-IV-C Rating Scale # 6160ChrisОценок пока нет
- Is It ADHD or Autism or BothДокумент4 страницыIs It ADHD or Autism or BothTony Blair100% (1)
- CCC Adhd TestingДокумент6 страницCCC Adhd TestingAnnisa Chaerani Burhanuddin100% (1)
- The Assessment of Executive Functioning in ChildrenДокумент37 страницThe Assessment of Executive Functioning in ChildrenYovana Estefany Lasso Caicedo100% (1)
- Tips Managing Adhd in ClassДокумент2 страницыTips Managing Adhd in ClassSobahОценок пока нет
- ASD Assessment by Age Best Practice 638466 7Документ8 страницASD Assessment by Age Best Practice 638466 7Aggelou Maya50% (2)
- ADHD Workshop FlyerДокумент1 страницаADHD Workshop Flyerhengland9406Оценок пока нет
- The Parent Teacher HandbookДокумент76 страницThe Parent Teacher HandbookAdrian Gt50% (2)
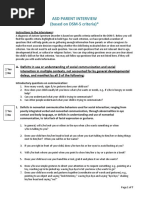
- Asd-Parent-Interview Formatted 2012 0325 PDFДокумент7 страницAsd-Parent-Interview Formatted 2012 0325 PDFVivek SagarОценок пока нет
- The Defiant Child: A Parent's Guide To Oppositional Defiant Disorder - Douglas A. RileyДокумент4 страницыThe Defiant Child: A Parent's Guide To Oppositional Defiant Disorder - Douglas A. RileysaxefewoОценок пока нет
- Preschool ADHD QuestionnaireДокумент2 страницыPreschool ADHD QuestionnaireLily Marlina100% (1)
- Assessment of Adult ADHDДокумент24 страницыAssessment of Adult ADHDPsydoc100% (4)
- Adult ADHD - Effective Treatment StrategiesДокумент15 страницAdult ADHD - Effective Treatment StrategiesDefault User100% (4)
- ADHD Parent HandbookДокумент9 страницADHD Parent HandbookDard Tong0% (1)
- Guidelines Adhd AdultДокумент19 страницGuidelines Adhd AdultJavier Cotobal100% (1)
- Ace PDFДокумент40 страницAce PDFjoel cuadra100% (1)
- Adhd Rating ScaleДокумент1 страницаAdhd Rating Scaleabu ubaidahОценок пока нет
- ADHD Conners Self-Report TeenДокумент3 страницыADHD Conners Self-Report TeenLisa HernandezОценок пока нет
- CaddraGuidelines2011 ToolkitДокумент48 страницCaddraGuidelines2011 ToolkitYet Barreda BasbasОценок пока нет
- Child Clinical Interview Form OnlineДокумент24 страницыChild Clinical Interview Form OnlineMonica Bolocan100% (3)
- Adhd A Guide For Parents: Understanding Attention Deficit Hyperactivity DisorderДокумент28 страницAdhd A Guide For Parents: Understanding Attention Deficit Hyperactivity DisorderMary Carmen Rodriguez100% (1)
- Diagnostic Tools For The Initial Evaluation of Adhd and Monitoring Treatment SuccessДокумент39 страницDiagnostic Tools For The Initial Evaluation of Adhd and Monitoring Treatment SuccessHR Agha Steel100% (1)
- ADHD Provider Toolkit - 2017 - FINALДокумент24 страницыADHD Provider Toolkit - 2017 - FINALblessy jonesОценок пока нет
- Modified Coventry Model - Including PDA ProfileДокумент13 страницModified Coventry Model - Including PDA ProfileAliens-and-antsОценок пока нет
- Guide To Assessment Scales in ADHD 2nd Ed. - S. Kollins, Et. Al., (Springer Hlthcare, 2010) WWДокумент65 страницGuide To Assessment Scales in ADHD 2nd Ed. - S. Kollins, Et. Al., (Springer Hlthcare, 2010) WWAntonio DoniniОценок пока нет
- The Basics: Introduction To Attention Deficit Symptoms, Diagnosis, and TreatmentДокумент16 страницThe Basics: Introduction To Attention Deficit Symptoms, Diagnosis, and TreatmentJeannette DorfmanОценок пока нет
- ADHD Therapy WorksheetДокумент22 страницыADHD Therapy Worksheetmizbigspenda100% (2)
- Adhd ManualДокумент72 страницыAdhd ManualJuwita Pratiwi100% (1)
- Aceplus EnglishДокумент44 страницыAceplus EnglishPirilloОценок пока нет
- ADHD AssessmentДокумент6 страницADHD AssessmentIlma SikandarОценок пока нет
- Executive Functioning - Advanced Assessment and InterpretationДокумент127 страницExecutive Functioning - Advanced Assessment and InterpretationTurfa Ahmed50% (2)
- Classroom Interventions For Attention Deficit/Hyperactivity DisorderДокумент10 страницClassroom Interventions For Attention Deficit/Hyperactivity DisorderanhiramdhaniОценок пока нет
- Adhd FlowplanДокумент6 страницAdhd Flowplanapi-343183708Оценок пока нет
- 3 Types of ADHD - Neurochemical MechanismsДокумент2 страницы3 Types of ADHD - Neurochemical MechanismsBrendha MОценок пока нет
- Adhd - Newsletter 1Документ4 страницыAdhd - Newsletter 1api-344792702Оценок пока нет
- Emotional Intelligence As An Evolutive Factor On Adult With ADHDДокумент9 страницEmotional Intelligence As An Evolutive Factor On Adult With ADHDDoctora Rosa Vera GarcíaОценок пока нет
- Inside The ADD Mind, by Dr. Thomas BrownДокумент4 страницыInside The ADD Mind, by Dr. Thomas BrownDerekОценок пока нет
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderДокумент2 страницыAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasОценок пока нет
- John Smith: PECS Example Comprehensive ADHD ReportДокумент33 страницыJohn Smith: PECS Example Comprehensive ADHD Reportgenerjustn100% (2)
- AdhdДокумент2 страницыAdhdapi-671375887Оценок пока нет
- Solanto - CBT For Adult ADHDДокумент31 страницаSolanto - CBT For Adult ADHDTamás Petőcz0% (1)
- Weiss Functional Impairment Rating Scale - Self Report (Wfirs-S)Документ2 страницыWeiss Functional Impairment Rating Scale - Self Report (Wfirs-S)Mariana LópezОценок пока нет
- B-BAARS English PDFДокумент10 страницB-BAARS English PDFAi SanОценок пока нет
- 10 Neurodiversity Affirming Principles For TherapistsДокумент1 страница10 Neurodiversity Affirming Principles For TherapistsBelegan CrengutaОценок пока нет
- Adhd Workshop Gpa 2016 041016c2Документ128 страницAdhd Workshop Gpa 2016 041016c2meiraimОценок пока нет
- DP - Adhd - DoneДокумент12 страницDP - Adhd - Doneapi-284988119Оценок пока нет
- A Psychoeducational and Support Group For Parents of ADD - ADHD ChiДокумент9 страницA Psychoeducational and Support Group For Parents of ADD - ADHD ChiTulaОценок пока нет
- Adultadhdscreenertest 1Документ3 страницыAdultadhdscreenertest 1FAKESIGNUPACCOUNTОценок пока нет
- Special ReportДокумент8 страницSpecial ReportAndrii DutkoОценок пока нет
- Scanned by TapscannerДокумент3 страницыScanned by TapscannerFreditya Mahendra PutraОценок пока нет
- Surat Izin OrtuДокумент1 страницаSurat Izin OrtuFreditya Mahendra PutraОценок пока нет
- 5 6100542719417910010Документ21 страница5 6100542719417910010Freditya Mahendra PutraОценок пока нет
- Regional Obstetric Early Warning Score ChartДокумент4 страницыRegional Obstetric Early Warning Score ChartFreditya Mahendra PutraОценок пока нет
- DATA KARYAWAN Disnaker Fix PDFДокумент60 страницDATA KARYAWAN Disnaker Fix PDFFreditya Mahendra PutraОценок пока нет
- Effects of Alcohol, Tobacco, and Marijuana - PR 1Документ11 страницEffects of Alcohol, Tobacco, and Marijuana - PR 1Mark Andris GempisawОценок пока нет
- Stroke Practice GuidelineДокумент274 страницыStroke Practice GuidelineCamila HernandezОценок пока нет
- 2022BusinessManagement ReportДокумент17 страниц2022BusinessManagement ReportkianaОценок пока нет
- Chan Sophia ResumeДокумент1 страницаChan Sophia Resumeapi-568119902Оценок пока нет
- IUGRДокумент4 страницыIUGRMichael Spica RampangileiОценок пока нет
- 115 FinargДокумент294 страницы115 FinargMelvin GrijalbaОценок пока нет
- Olinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Документ4 страницыOlinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Justia.comОценок пока нет
- Bossa Nova Book PDFДокумент5 страницBossa Nova Book PDFschmimiОценок пока нет
- (Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFДокумент451 страница(Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFnlf2205100% (3)
- Ang Tibay Vs CAДокумент2 страницыAng Tibay Vs CAEarl LarroderОценок пока нет
- Corporation Law Case Digests Philippines Merger and ConsolidationДокумент7 страницCorporation Law Case Digests Philippines Merger and ConsolidationAlpha BetaОценок пока нет
- Paradigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportДокумент5 страницParadigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportPsychology and Education: A Multidisciplinary JournalОценок пока нет
- AmplifierДокумент20 страницAmplifierValerie StraussОценок пока нет
- Role of Courts in Granting Bails and Bail Reforms: TH THДокумент1 страницаRole of Courts in Granting Bails and Bail Reforms: TH THSamarth VikramОценок пока нет
- Malefactor ClassДокумент23 страницыMalefactor ClassMatthew Duncan100% (6)
- Aìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutДокумент28 страницAìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDāmodar DasОценок пока нет
- Debus Medical RenaissanceДокумент3 страницыDebus Medical RenaissanceMarijaОценок пока нет
- History of The UST School of Fine Arts, Chapter 4Документ27 страницHistory of The UST School of Fine Arts, Chapter 4Hannibal F. CaradoОценок пока нет
- Final Paper IN MAJOR 14 EL 116 Life and Death: Fear Reflected in John Green's The Fault in Our StarsДокумент12 страницFinal Paper IN MAJOR 14 EL 116 Life and Death: Fear Reflected in John Green's The Fault in Our StarsMary Rose FragaОценок пока нет
- IB Math Studies - Triangle Trigonometry Practice Key: MarkschemeДокумент45 страницIB Math Studies - Triangle Trigonometry Practice Key: MarkschemeRafael Tayo0% (1)
- Customer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsДокумент12 страницCustomer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsAziz KhanОценок пока нет
- SAP CRM Tax ConfigurationДокумент18 страницSAP CRM Tax Configurationtushar_kansaraОценок пока нет
- Aruego, Jr. v. Court of Appeals, G.R. No. 112193, March 13, 1996Документ5 страницAruego, Jr. v. Court of Appeals, G.R. No. 112193, March 13, 1996hello kitty black and whiteОценок пока нет
- Rectification or Correction of Sale DeedДокумент4 страницыRectification or Correction of Sale Deedsumanth_0678Оценок пока нет
- 1929 Davos DisputationДокумент20 страниц1929 Davos DisputationEstevao Cruz100% (1)
- Names of AllahДокумент8 страницNames of AllahAfshaan BanuОценок пока нет
- Lesson I. Background InformationДокумент21 страницаLesson I. Background InformationsuidivoОценок пока нет
- STEM BeesДокумент36 страницSTEM BeesHitesh YadavОценок пока нет
- American RunwayДокумент26 страницAmerican RunwayGayathri SuriyaОценок пока нет
- WHO CDS HIV 19.8 EngДокумент24 страницыWHO CDS HIV 19.8 EngMaykel MontesОценок пока нет