Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Halc 1Документ72 страницыHalc 1Indra MishraОценок пока нет
- Intermodal Vs Multimodal TransportationДокумент6 страницIntermodal Vs Multimodal TransportationJanice ThomasОценок пока нет
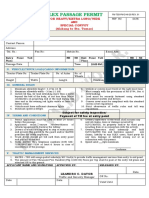
- Passage PermitДокумент1 страницаPassage PermitYG GOLD100% (1)
- Speed Twin Clutch DSG S - Tronic AudiДокумент88 страницSpeed Twin Clutch DSG S - Tronic Audikepler2775% (4)
- Turfgrid: Versatile Permeable PavementДокумент2 страницыTurfgrid: Versatile Permeable PavementBenОценок пока нет
- SP 168 DДокумент8 страницSP 168 DHarlinton descalziОценок пока нет
- Borrow Material MethodologyДокумент15 страницBorrow Material MethodologyMusenge MusengeОценок пока нет
- 2020 Great Aloha Run Road ClosuresДокумент2 страницы2020 Great Aloha Run Road ClosuresHNN100% (1)
- Case Digest Sps Perena V Sps NicolasДокумент3 страницыCase Digest Sps Perena V Sps NicolasJem LicanoОценок пока нет
- Lecture On Env Impact of TransportationДокумент40 страницLecture On Env Impact of TransportationMuhannad Al ManwariОценок пока нет
- P6 Project Master Schedule - Roads PDFДокумент1 страницаP6 Project Master Schedule - Roads PDFengsam777Оценок пока нет
- Bellville Public Transport InterchangeДокумент118 страницBellville Public Transport InterchangeJulieОценок пока нет
- QAQCДокумент56 страницQAQCRavindra Babu Sivapu100% (1)
- DL & SIDL Calculation (NH-130A)Документ18 страницDL & SIDL Calculation (NH-130A)amitОценок пока нет
- Draft of A Research Proposal On Mobility Data and Traffic Demand in The Town of OngwedivaДокумент9 страницDraft of A Research Proposal On Mobility Data and Traffic Demand in The Town of OngwedivaSt3f1e100% (1)
- New RPP04 BFC32302 Sem 1 2019 2020Документ4 страницыNew RPP04 BFC32302 Sem 1 2019 2020ElilragiGanasan0% (1)
- Final VehiclesДокумент35 страницFinal VehiclesFaizrul YusoffОценок пока нет
- RHD Management Manual Vol-1Документ93 страницыRHD Management Manual Vol-1Sadia Hossain DristiОценок пока нет
- Ecil Model Paper: Expected Model Pattern For The Entrance Exam of ECIL GET Is As BelowcДокумент9 страницEcil Model Paper: Expected Model Pattern For The Entrance Exam of ECIL GET Is As BelowcSumit KumarОценок пока нет
- Mountain Bike Kathmandu To Pokhara: 11 Days/10 Nights Departure DatesДокумент6 страницMountain Bike Kathmandu To Pokhara: 11 Days/10 Nights Departure DatesChris StaalОценок пока нет
- Carrollton Trail MapДокумент2 страницыCarrollton Trail MapspohnheimerОценок пока нет
- Compensation Under Motor Vehicle Act, 1988Документ19 страницCompensation Under Motor Vehicle Act, 1988Shristi TalukdarОценок пока нет
- BMW StarMarkedTiresДокумент2 страницыBMW StarMarkedTiresMohsenMostafaОценок пока нет
- Rigid Pavement Design PDFДокумент14 страницRigid Pavement Design PDFvikashОценок пока нет
- Index of DrawingДокумент1 страницаIndex of Drawingjc aremeroОценок пока нет
- Transportation Modes, Modal Competition and Modal ShiftДокумент41 страницаTransportation Modes, Modal Competition and Modal ShiftAhmed Saeed SoudyОценок пока нет
- Manipal Hospital Final PPT 2Документ15 страницManipal Hospital Final PPT 2sqytОценок пока нет
- Pala Cargadora 835hДокумент2 страницыPala Cargadora 835hRoxana Alvarez VerduguezОценок пока нет
- Responding To HorrorДокумент111 страницResponding To Horrorstuarthwyman100% (1)
- Amkus Rescue StrutsДокумент2 страницыAmkus Rescue StrutsForum PompieriiОценок пока нет