Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Sattler-Assessment of Children PDFДокумент67 страницSattler-Assessment of Children PDFTakashi Aoki100% (6)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- 5 Feet Apart - ScriptДокумент40 страниц5 Feet Apart - ScriptJay100% (1)
- Sonography Scanning Principles and Protocols Ultrasound Scanning 4th Edition Ebook PDF VersionДокумент62 страницыSonography Scanning Principles and Protocols Ultrasound Scanning 4th Edition Ebook PDF Versionroland.bell57698% (41)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Critical Practice in Social WorkДокумент381 страницаCritical Practice in Social WorkMarko MitrovicОценок пока нет
- Jurnal RukasinДокумент13 страницJurnal RukasinAlvin RinaldoОценок пока нет
- COVID-19 Alvin RinaldoДокумент21 страницаCOVID-19 Alvin RinaldoAlvin RinaldoОценок пока нет
- Pemicu 4 AlvinДокумент63 страницыPemicu 4 AlvinAlvin RinaldoОценок пока нет
- Approach To Jundiced PatientДокумент2 страницыApproach To Jundiced Patientmelinda SilalahiОценок пока нет
- Shi 2019Документ9 страницShi 2019Alvin RinaldoОценок пока нет
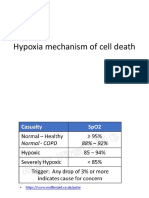
- Hypoxia Mechanism of Cell DeathДокумент4 страницыHypoxia Mechanism of Cell DeathAlvin RinaldoОценок пока нет
- Finecare 114Документ2 страницыFinecare 114lumira BogotaОценок пока нет
- Emergency ProceduresДокумент6 страницEmergency Proceduresumamaheswara reddy BonthuОценок пока нет
- Language Review 3Документ4 страницыLanguage Review 3Walaa WalaaОценок пока нет
- Pharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Документ11 страницPharmaceutical Development Q8 (R2) : International Conference On Harmonisation (ICH)Md. Akil Mahmud100% (1)
- DM 2021-0330 Reverse Logistics Commissioned To Integrated Waste Management IncДокумент3 страницыDM 2021-0330 Reverse Logistics Commissioned To Integrated Waste Management IncCharlie ManilaОценок пока нет
- Risk Management (Starbucks) G3Документ8 страницRisk Management (Starbucks) G3Chaddy Kayle MimbalawagОценок пока нет
- Warm Up For TaekwondoДокумент8 страницWarm Up For TaekwondoAki ZamiraОценок пока нет
- Resume - Hourvash Ebrahimi LouyehДокумент3 страницыResume - Hourvash Ebrahimi Louyeharian tejaratОценок пока нет
- Banco de Preguntas ReabilitacionДокумент19 страницBanco de Preguntas ReabilitacionVanessa AlcantaraОценок пока нет
- The Human Person Flourishing in Science and TechnologyДокумент40 страницThe Human Person Flourishing in Science and TechnologyMary Grace V. PeñalbaОценок пока нет
- Aichi Medical GroupДокумент7 страницAichi Medical GroupEast West Medical College & HospitalОценок пока нет
- Effects of Green Tea On Periodontal Health: A Prospective Clinical StudyДокумент7 страницEffects of Green Tea On Periodontal Health: A Prospective Clinical StudyBanyu علي تقويم BiruОценок пока нет
- EOBI Pension Calculation Formula in ExcelДокумент4 страницыEOBI Pension Calculation Formula in ExcelAdeelОценок пока нет
- 0092015020Документ9 страниц0092015020ChloéОценок пока нет
- Questions of HSE Competency AssessmentДокумент16 страницQuestions of HSE Competency AssessmentekoimampОценок пока нет
- Ammonia & Ammonia Solution STORAGE AND HANDLINGДокумент28 страницAmmonia & Ammonia Solution STORAGE AND HANDLINGmah_abdelaalОценок пока нет
- 3003-214 l2 Logbook Downloadable Unit v1 PDFДокумент12 страниц3003-214 l2 Logbook Downloadable Unit v1 PDFAlexis O'SullivanОценок пока нет
- Thomson Medical PTE LTD Corporate Social Responsibility InitiativesДокумент5 страницThomson Medical PTE LTD Corporate Social Responsibility InitiativesElias MwangiОценок пока нет
- Propylthiouracil 2Документ14 страницPropylthiouracil 2Magdy Ali ELsherbenyОценок пока нет
- Material Safety Data Sheet Polivis PWДокумент4 страницыMaterial Safety Data Sheet Polivis PWfs1640Оценок пока нет
- 2 Manual de Seguridad en ExcavacionesДокумент40 страниц2 Manual de Seguridad en ExcavacionesJaime Leon NoriegaОценок пока нет
- Muhammad Ismail - Workstyle Personality Questionnaire (WPQ) - 2325596Документ3 страницыMuhammad Ismail - Workstyle Personality Questionnaire (WPQ) - 2325596Hafiz Saddique MalikОценок пока нет
- HousekeepingДокумент18 страницHousekeepingমুসফেকআহমেদনাহিদОценок пока нет
- Siddha Medicine For BronchitisДокумент2 страницыSiddha Medicine For BronchitisGokul SmartОценок пока нет
- Customer Care and Communication SkillsДокумент59 страницCustomer Care and Communication SkillshemedОценок пока нет
- Instructions For A Bad Day - Dhanvi AgarwalДокумент4 страницыInstructions For A Bad Day - Dhanvi Agarwalapi-518570746Оценок пока нет