Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Therapeutic EffectsofWhole-BodyDevices Applying Pulsed Electromagnetic Fields (PEMF)Документ11 страницTherapeutic EffectsofWhole-BodyDevices Applying Pulsed Electromagnetic Fields (PEMF)Jeroan MonteiroОценок пока нет
- Wireline Works Tech-BulletinsДокумент25 страницWireline Works Tech-BulletinsRio de Mario100% (1)
- Introduction To PercolationДокумент25 страницIntroduction To Percolationpasomaga100% (1)
- OSTEOARTHRITISДокумент53 страницыOSTEOARTHRITISRiza Umami100% (1)
- Soal B.inggris Kelas 2Документ3 страницыSoal B.inggris Kelas 2Riza Umami100% (4)
- Soal B.inggris Kelas 2Документ3 страницыSoal B.inggris Kelas 2Riza Umami100% (4)
- Novi MASSAGEДокумент10 страницNovi MASSAGERiza UmamiОценок пока нет
- Effect of Personal and Work Stress On Burnout, JobДокумент7 страницEffect of Personal and Work Stress On Burnout, JobEng-Mohammed Abu NuktaОценок пока нет
- Novi MASSAGEДокумент10 страницNovi MASSAGERiza UmamiОценок пока нет
- PRD Doc Pro 3201-00001 Sen Ain V31Документ10 страницPRD Doc Pro 3201-00001 Sen Ain V31rudybestyjОценок пока нет
- Sentinel Visualizer 6 User GuideДокумент227 страницSentinel Visualizer 6 User GuideTaniaОценок пока нет
- KVS - Regional Office, JAIPUR - Session 2021-22Документ24 страницыKVS - Regional Office, JAIPUR - Session 2021-22ABDUL RAHMAN 11BОценок пока нет
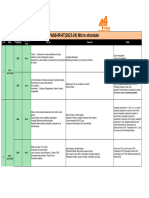
- Narayana Xii Pass Ir Iit (2023 24) PDFДокумент16 страницNarayana Xii Pass Ir Iit (2023 24) PDFRaghav ChaudharyОценок пока нет
- I C Engine LabДокумент3 страницыI C Engine LabDevОценок пока нет
- Excel NotesДокумент9 страницExcel NotesAhnОценок пока нет
- SR-X Script Reference - EДокумент24 страницыSR-X Script Reference - EDomagoj ZagoracОценок пока нет
- Chem 1211 Lab ReportДокумент9 страницChem 1211 Lab Reportansleybarfield0% (1)
- VT300 User ManualДокумент21 страницаVT300 User ManualLuvОценок пока нет
- Magnetism NotesДокумент14 страницMagnetism Notesapi-277818647Оценок пока нет
- Mechanism of Muscle ContractionДокумент24 страницыMechanism of Muscle Contractionfisika100% (1)
- Translating Trig Graphs PDFДокумент4 страницыTranslating Trig Graphs PDFMark Abion ValladolidОценок пока нет
- Cópia de Teste Excel - Intermediário (5166) .XLS: BIM Technology For EngineersДокумент6 страницCópia de Teste Excel - Intermediário (5166) .XLS: BIM Technology For EngineersFernanda AzevedoОценок пока нет
- Network Command - HPUXДокумент5 страницNetwork Command - HPUXRashid NihalОценок пока нет
- Chapter 19. TemperatureДокумент41 страницаChapter 19. TemperatureNguyên Nguyễn SơnОценок пока нет
- Servodisc CatalogДокумент87 страницServodisc CatalogEstebanRojasKrustofskyОценок пока нет
- North Sails Brochure 2007 enДокумент24 страницыNorth Sails Brochure 2007 ennorthsailsОценок пока нет
- A Comparative Study On The Academic Performance ofДокумент18 страницA Comparative Study On The Academic Performance ofDiether Allen L. YnionОценок пока нет
- 307-01 Automatic Transmission 10 Speed - Description and Operation - DescriptionДокумент12 страниц307-01 Automatic Transmission 10 Speed - Description and Operation - DescriptionCARLOS LIMADAОценок пока нет
- PythagorasДокумент109 страницPythagorasaditya00012Оценок пока нет
- Analysis and Design of Telecommunication Tower Using Different Truss System by ETab SoftwareДокумент12 страницAnalysis and Design of Telecommunication Tower Using Different Truss System by ETab SoftwareEditor IJTSRDОценок пока нет
- University of Cambridge International Examinations General Certificate of Education Advanced LevelДокумент4 страницыUniversity of Cambridge International Examinations General Certificate of Education Advanced LevelHubbak KhanОценок пока нет
- Chapter 3Документ23 страницыChapter 3pganoelОценок пока нет
- Trigonometric Ratios LPДокумент3 страницыTrigonometric Ratios LPjoshgarciadlt100% (2)
- New Features in IbaPDA v7.1.0Документ39 страницNew Features in IbaPDA v7.1.0Miguel Ángel Álvarez VázquezОценок пока нет
- Microporous and Mesoporous Materials: SciencedirectДокумент8 страницMicroporous and Mesoporous Materials: SciencedirectAssyakurОценок пока нет
- List of GHS Hazard Statement & PictogramsДокумент33 страницыList of GHS Hazard Statement & PictogramsKhairul BarsriОценок пока нет