Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Dysmenorrhoea PDFДокумент7 страницDysmenorrhoea PDFRafiqy Sa'adiy FaizunОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
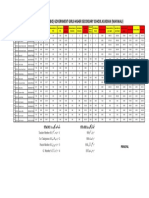
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Документ1 страницаMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadОценок пока нет
- Characteristics of Gay, Bisexual and Other Men Who.1 PDFДокумент6 страницCharacteristics of Gay, Bisexual and Other Men Who.1 PDFGvidas MikalauskasОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Brevard County Breastfeeding Resourcesjan2016Документ2 страницыBrevard County Breastfeeding Resourcesjan2016api-250832672Оценок пока нет
- Male Sex DisordersДокумент2 страницыMale Sex DisordersAR LOОценок пока нет
- Notes On Subfertility AssessmentДокумент5 страницNotes On Subfertility AssessmentHassen ZabalaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Intrauterine Device - WikipediaДокумент80 страницIntrauterine Device - WikipediaDarshan MvОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Abortion Should Not Be Used As An Alternative To ContraceptionДокумент4 страницыAbortion Should Not Be Used As An Alternative To Contraceptionjaimin100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Bishop's ScoreДокумент2 страницыBishop's ScoreAndy WijayaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Understanding The Self (Report)Документ53 страницыUnderstanding The Self (Report)Jaymark S. GicaleОценок пока нет
- Surrogacy Law in IndiaДокумент29 страницSurrogacy Law in IndiaKanak Singh100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Live OR Survive?: Narvaez, Amiel Harold G. Section 147Документ15 страницLive OR Survive?: Narvaez, Amiel Harold G. Section 147Aaron CabiaОценок пока нет
- Natural Science. Level 6. Unit 3. ReproductionДокумент3 страницыNatural Science. Level 6. Unit 3. ReproductionAna Rosa Camacho Cornejo50% (2)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Reproductive Health Udaan Dpp1Документ14 страницReproductive Health Udaan Dpp1noobОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Assisted Reproductive Techniques For Class 12 Investigatory ProjectДокумент9 страницAssisted Reproductive Techniques For Class 12 Investigatory Projectjerusha50% (6)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Infertility: A Presentation Of: Romuelle Barbado Bea Transfiguracion Allison Ellano Mark Dovie DionioДокумент30 страницInfertility: A Presentation Of: Romuelle Barbado Bea Transfiguracion Allison Ellano Mark Dovie DioniobesprenОценок пока нет
- Bad Girl's Bible BDSM ChecklistДокумент11 страницBad Girl's Bible BDSM ChecklistAth slave100% (1)
- SpeechДокумент3 страницыSpeechBoy Kakak Toki100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Why Is The Church Against The RH BillДокумент2 страницыWhy Is The Church Against The RH BillDenise Kimberly GoОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Contraception Chart SexualityДокумент8 страницContraception Chart SexualityRNStudent1Оценок пока нет
- Sex 1Документ3 страницыSex 1keroОценок пока нет
- Comparison Between Intrauterine Insemination With Ovulation Induction Versus Natural Ovulatory Cycle in Male Factor of InfertilityДокумент74 страницыComparison Between Intrauterine Insemination With Ovulation Induction Versus Natural Ovulatory Cycle in Male Factor of InfertilityMohammed Ahmed AzabОценок пока нет
- 15 Best KamaSutra TechniquesДокумент19 страниц15 Best KamaSutra TechniquesSwati Gosh100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Abortion DebateДокумент18 страницThe Abortion DebatePat Abrosa AmkayahОценок пока нет
- Pictures of Six Sexual Transmitted InfectionДокумент6 страницPictures of Six Sexual Transmitted InfectionDavia ColmanОценок пока нет
- A American Sex SurveyДокумент27 страницA American Sex SurveyRamesh RajagopalanОценок пока нет
- Mks Notes in Obgyn eДокумент134 страницыMks Notes in Obgyn eإسراء محمود100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Sex EducationДокумент18 страницSex EducationRoshni Mahapatra80% (5)
- BDSM Checklist PDFДокумент6 страницBDSM Checklist PDFLauraGabrielaBonteaОценок пока нет
- Facts About Abstinence: 8.3 Work FileДокумент4 страницыFacts About Abstinence: 8.3 Work FileAaron Alam33% (3)