Вам также может понравиться
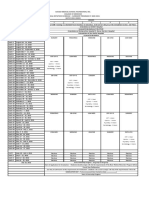
- Davao Medical School Foundation, Inc. College of Medicine Clinical Rotation Schedule - Clerkship Program Sy 2020-2021 BATCH 2021 (NMD) DateДокумент1 страницаDavao Medical School Foundation, Inc. College of Medicine Clinical Rotation Schedule - Clerkship Program Sy 2020-2021 BATCH 2021 (NMD) DateJxyp MundoОценок пока нет
- Final IM CaseДокумент9 страницFinal IM CaseJxyp MundoОценок пока нет
- OB 2nd SGDДокумент4 страницыOB 2nd SGDJxyp MundoОценок пока нет
- Mundo - Ob Case 1Документ6 страницMundo - Ob Case 1Jxyp MundoОценок пока нет
- Case Presentation SleДокумент33 страницыCase Presentation SleJxyp MundoОценок пока нет
- Mundo - Ob Case 1Документ6 страницMundo - Ob Case 1Jxyp MundoОценок пока нет
- Anxiety and Personality Disorder PDFДокумент88 страницAnxiety and Personality Disorder PDFJxyp MundoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- MCQ Biomechanics of Hip JointДокумент16 страницMCQ Biomechanics of Hip Jointdrng48100% (9)
- Anatomy of The Hand: Khalid AyoubДокумент53 страницыAnatomy of The Hand: Khalid Ayoubvaikunthan100% (2)
- Herniated Disk in The Lower Back: AnatomyДокумент6 страницHerniated Disk in The Lower Back: AnatomyLate ArtistОценок пока нет
- LaVoy Finicum Autopsy Report, Jan 28, 2016Документ13 страницLaVoy Finicum Autopsy Report, Jan 28, 2016John SutherlandОценок пока нет
- 41ch44circulatory12008 RevisedДокумент33 страницы41ch44circulatory12008 RevisedJosh TejadaОценок пока нет
- BFO - AnatomyДокумент33 страницыBFO - AnatomynovitaОценок пока нет
- Chapter 1 - Practical Notions Concerning Dental Occlusion: Personal InformationДокумент61 страницаChapter 1 - Practical Notions Concerning Dental Occlusion: Personal InformationEmil Costruț100% (1)
- The Essential Review Guide For Passing The Mblex Licensing Exam 2017 EditionДокумент192 страницыThe Essential Review Guide For Passing The Mblex Licensing Exam 2017 EditionSabrina Marie100% (3)
- Checklist Cardiac AssessmentДокумент8 страницChecklist Cardiac AssessmentLovely GopezОценок пока нет
- Thyroid Function TestsДокумент9 страницThyroid Function Testsmdowl90Оценок пока нет
- Muscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Документ9 страницMuscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Rishbha TikuОценок пока нет
- Autopsy: Forensic Medicine & Toxicology, NMCДокумент106 страницAutopsy: Forensic Medicine & Toxicology, NMCAiman sadiq shahОценок пока нет
- Set Up. Download. Workout.: Ready To Sweat? Let'S GoДокумент24 страницыSet Up. Download. Workout.: Ready To Sweat? Let'S GoDavid HavensОценок пока нет
- Human Body PDFДокумент9 страницHuman Body PDFAnonymous W4MMefmCОценок пока нет
- Tanveer Notes Revised 1st ED (Uploaded by Hanan)Документ102 страницыTanveer Notes Revised 1st ED (Uploaded by Hanan)jawad100% (4)
- Caffey's Pediatric Diagnostic ImagingДокумент8 страницCaffey's Pediatric Diagnostic ImagingHafiz DjosanОценок пока нет
- Histology of GitДокумент31 страницаHistology of GitLucky LuckyОценок пока нет
- All Important Diagrams Class 10 (Prashant Kirad) PDFДокумент39 страницAll Important Diagrams Class 10 (Prashant Kirad) PDFharshita1934100% (1)
- Genicular Nerves BlockДокумент14 страницGenicular Nerves BlocknsatriotomoОценок пока нет
- Free Preview: ShouldersДокумент21 страницаFree Preview: ShouldersSiva SubramanianОценок пока нет
- Compositae FamilyДокумент23 страницыCompositae FamilyA.H. Lammert Holdijk100% (1)
- NCMA121.HAs - RLE PHYSICAL ASSESSMENT ADULT PART 1Документ3 страницыNCMA121.HAs - RLE PHYSICAL ASSESSMENT ADULT PART 1Rowena SamsonОценок пока нет
- Anatomy Past Papers 2009-2019Документ12 страницAnatomy Past Papers 2009-2019Kashar SaeedОценок пока нет
- Classification of MalocclusionДокумент69 страницClassification of MalocclusionBatman 02053Оценок пока нет
- Booty X Body BoostДокумент4 страницыBooty X Body BoostMr SОценок пока нет
- Anatomy of An EyeДокумент66 страницAnatomy of An EyeChoco VaniОценок пока нет
- Past QuestionsДокумент116 страницPast QuestionsYhr YhОценок пока нет
- Gym PrinciplesДокумент23 страницыGym PrinciplesKrešimir DodigОценок пока нет
- Xrug7152 1 PDFДокумент2 страницыXrug7152 1 PDFSarah ArpithaОценок пока нет
- Oral Anatomy Q&AДокумент8 страницOral Anatomy Q&AHanny CarinoОценок пока нет