Вам также может понравиться
- FNCP NearДокумент29 страницFNCP NearAl LimОценок пока нет
- Family Nursing Care Plan G4 BSN2 4 DonДокумент31 страницаFamily Nursing Care Plan G4 BSN2 4 DonStuart BlackОценок пока нет
- Malnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredДокумент1 страницаMalnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredSareno PJhēaОценок пока нет
- Family Nursing Care Plan for Hypertension ManagementДокумент3 страницыFamily Nursing Care Plan for Hypertension ManagementBiway RegalaОценок пока нет
- Abc NCPДокумент3 страницыAbc NCPKL AstudilloОценок пока нет
- Family Nursing Process: Initial DatabaseДокумент39 страницFamily Nursing Process: Initial DatabaseMariz Joy Gonzales Guillermo100% (1)
- Second Level AssessmentДокумент4 страницыSecond Level AssessmentPixel DinibitОценок пока нет
- Water Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationДокумент2 страницыWater Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationlovlyОценок пока нет
- Family Nursing Care Plan for Improving HygieneДокумент5 страницFamily Nursing Care Plan for Improving HygieneCLARENCE REMUDAROОценок пока нет
- FNCPДокумент1 страницаFNCPThunderОценок пока нет
- Family Nursing Care Plan Prioritization and InterventionДокумент15 страницFamily Nursing Care Plan Prioritization and InterventionLouis Gabriel AdayaОценок пока нет
- FNCPДокумент9 страницFNCPJesse UliganОценок пока нет
- FNCP NotesДокумент13 страницFNCP NotesAmiel Francisco ReyesОценок пока нет
- vINA Faulty Eating HabitsДокумент2 страницыvINA Faulty Eating HabitsMyrshaida IbrahimОценок пока нет
- Malnutrition FNCPДокумент3 страницыMalnutrition FNCPMaribel ValenzuelaОценок пока нет
- FNCP Risk For InfectionДокумент4 страницыFNCP Risk For InfectionAemz Alacasnap Ainegud0% (1)
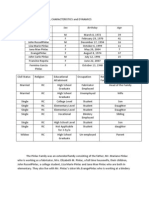
- Family Structure: A., Characteristics and DynamicsДокумент4 страницыFamily Structure: A., Characteristics and DynamicsZerrie lei HartОценок пока нет
- Group #4: Unit Task #1 (Nursing Research I)Документ11 страницGroup #4: Unit Task #1 (Nursing Research I)AriaОценок пока нет
- Family Nursing Care PlanДокумент50 страницFamily Nursing Care PlanE.R.OОценок пока нет
- POST NATAL FNCP - DotdotДокумент1 страницаPOST NATAL FNCP - DotdotGiselle EstoquiaОценок пока нет
- 87% of Animals Does Not Have Anti-Rabies Injection: GoalДокумент3 страницы87% of Animals Does Not Have Anti-Rabies Injection: GoalDan HizonОценок пока нет
- Nutrition Education for an Underweight InfantДокумент2 страницыNutrition Education for an Underweight InfantYzobel Phoebe ParoanОценок пока нет
- Family Nursing Analysis LatestДокумент143 страницыFamily Nursing Analysis LatestLyca Mae AurelioОценок пока нет
- FAMILY NURSING CARE PLANДокумент3 страницыFAMILY NURSING CARE PLANSoniaMarieBalanayОценок пока нет
- Family nursing goal of care on proper food storageДокумент2 страницыFamily nursing goal of care on proper food storagekarl montanoОценок пока нет
- FNCP Healh Teaching CommunityДокумент14 страницFNCP Healh Teaching CommunityGabrielle CaicdoyОценок пока нет
- DOCUMENT Prioritizing Family Health ProblemsДокумент5 страницDOCUMENT Prioritizing Family Health ProblemsShane TamilОценок пока нет
- Criteria Computation Score JustificationДокумент5 страницCriteria Computation Score JustificationCharm JavierОценок пока нет
- Family Nursing Care PlanДокумент3 страницыFamily Nursing Care PlanMhikou HirabaroОценок пока нет
- Guide in Making The FCA 1Документ18 страницGuide in Making The FCA 1Zedrake CaraanОценок пока нет
- Doroin Family Health Problems Ranking ScaleДокумент1 страницаDoroin Family Health Problems Ranking Scaleエド パジャロンОценок пока нет
- Family Nursing Care Plan FinalДокумент4 страницыFamily Nursing Care Plan Finalpanjerome100% (2)
- Drug StudyДокумент4 страницыDrug StudyDanica AbayaОценок пока нет
- Family Nursing Care Plan: "Hindi Kasi Uso Sa Kanila Yung Family Planning Eh "Документ2 страницыFamily Nursing Care Plan: "Hindi Kasi Uso Sa Kanila Yung Family Planning Eh "Jonver David0% (1)
- Kat PrioДокумент2 страницыKat PrioKatyana CesarОценок пока нет
- Adolescent NCPДокумент1 страницаAdolescent NCPClaire DobleОценок пока нет
- Post-abortion pain relief guideДокумент7 страницPost-abortion pain relief guideABDULRAHMAN MISHARI AL-THABITОценок пока нет
- FNCP PoorsanitationmarwahДокумент3 страницыFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahОценок пока нет
- Menopause As A Foreseeable Crisis: Nature of The ProblemДокумент2 страницыMenopause As A Foreseeable Crisis: Nature of The ProblemLouwella RamosОценок пока нет
- 1st Level Assessment JAVIER FOR STA CRUZ CASEДокумент4 страницы1st Level Assessment JAVIER FOR STA CRUZ CASEAndee SalegonОценок пока нет
- Total Population Number of Households A. Family Members and CharacteristicsДокумент20 страницTotal Population Number of Households A. Family Members and CharacteristicsDenvicОценок пока нет
- Problem # 3: Threat of Cross Infection From A Communicable Disease CaseДокумент3 страницыProblem # 3: Threat of Cross Infection From A Communicable Disease CaseRolandОценок пока нет
- FNCPДокумент30 страницFNCPAJ S Nvrro100% (1)
- Hypertension and Arthritis Health IssuesДокумент8 страницHypertension and Arthritis Health IssuesEunika Castro GarcesОценок пока нет
- FNCPДокумент2 страницыFNCPJaylove CastilloОценок пока нет
- A Family Nursing Care Plan OnДокумент14 страницA Family Nursing Care Plan OnMonique LeonardoОценок пока нет
- Planning FNCP Module-2.Canvas PDFДокумент16 страницPlanning FNCP Module-2.Canvas PDFms RNОценок пока нет
- Cytotec® Misoprostol TabletsДокумент12 страницCytotec® Misoprostol Tabletssuhandi71Оценок пока нет
- Case Study NCPДокумент4 страницыCase Study NCPKelly OstolОценок пока нет
- Breathing PatternДокумент4 страницыBreathing PatternVince John SevillaОценок пока нет
- Medical Management For PneumoniaДокумент2 страницыMedical Management For PneumoniaSue Elaine100% (1)
- Verbalized The Importance of Adequately Providing Intake of Nutritious Food To Pregnant WomenДокумент3 страницыVerbalized The Importance of Adequately Providing Intake of Nutritious Food To Pregnant WomenPeetah PanОценок пока нет
- FNCP Final EditedДокумент10 страницFNCP Final EditedMrLarry DolorОценок пока нет
- Family Coping Index AssessmentДокумент2 страницыFamily Coping Index AssessmentChloé Jane HilarioОценок пока нет
- Family Nursing Care Plan SampleДокумент2 страницыFamily Nursing Care Plan SampleKhylamarie VillalunaОценок пока нет
- FHNCP - PalmaДокумент4 страницыFHNCP - Palmachardy101100% (1)
- FNCP HyperacidityДокумент2 страницыFNCP HyperacidityJeriel DelavinОценок пока нет
- Eto Na FNCPДокумент96 страницEto Na FNCPCastillo EmilyОценок пока нет
- FCA Problem IdentificationДокумент8 страницFCA Problem IdentificationKenji CadizОценок пока нет
- Family Case Study-4Документ15 страницFamily Case Study-4Erl Joy Montaño Cañete100% (1)
- Integrating HUMSS Learning in Community ProjectsДокумент2 страницыIntegrating HUMSS Learning in Community ProjectsCaurrine MonsaludОценок пока нет
- CHAPTER - 3 - MSWORD - Do6cx Filename - UTF-8''CHAPTER 3 MSWORDДокумент8 страницCHAPTER - 3 - MSWORD - Do6cx Filename - UTF-8''CHAPTER 3 MSWORDCaurrine MonsaludОценок пока нет
- IntroductionДокумент4 страницыIntroductionCaurrine MonsaludОценок пока нет
- YyyyyДокумент2 страницыYyyyyCaurrine MonsaludОценок пока нет
- GenogramДокумент3 страницыGenogramCaurrine MonsaludОценок пока нет
- DrugsДокумент2 страницыDrugsCaurrine MonsaludОценок пока нет
- Methods of Contraception 1. Permanent ContraceptionДокумент7 страницMethods of Contraception 1. Permanent ContraceptionCaurrine MonsaludОценок пока нет
- HttpsДокумент7 страницHttpsCaurrine MonsaludОценок пока нет
- Drug Study (Pedia)Документ7 страницDrug Study (Pedia)Caurrine Monsalud100% (1)
- Comprehensive File of The Family Health InterventionsДокумент9 страницComprehensive File of The Family Health InterventionsCaurrine MonsaludОценок пока нет
- IntroductionДокумент4 страницыIntroductionCaurrine MonsaludОценок пока нет
- Comprehensive File of The Family Health InterventionsДокумент9 страницComprehensive File of The Family Health InterventionsCaurrine MonsaludОценок пока нет
- Nutrition Among AdolescentsДокумент9 страницNutrition Among AdolescentsCaurrine MonsaludОценок пока нет
- Nutrition Among AdolescentsДокумент9 страницNutrition Among AdolescentsCaurrine MonsaludОценок пока нет
- PoldsДокумент1 страницаPoldsCaurrine MonsaludОценок пока нет
- HEMODIALYSIS1Документ4 страницыHEMODIALYSIS1Caurrine MonsaludОценок пока нет
- Fetal Circulation and Placental StructuresДокумент2 страницыFetal Circulation and Placental StructuresCaurrine MonsaludОценок пока нет
- MONSALUDДокумент1 страницаMONSALUDCaurrine MonsaludОценок пока нет
- Readers Theater Life FlightДокумент5 страницReaders Theater Life FlightCaurrine Monsalud93% (14)
- HEMODIALYSIS1Документ4 страницыHEMODIALYSIS1Caurrine MonsaludОценок пока нет
- 123Документ2 страницы123Caurrine MonsaludОценок пока нет
- Factors Influencing Food HabitsДокумент3 страницыFactors Influencing Food HabitsCaurrine Monsalud100% (1)
- Brutas. ActivityДокумент14 страницBrutas. ActivityCaurrine MonsaludОценок пока нет
- 1Документ1 страница1Caurrine MonsaludОценок пока нет
- CHAPTER - 3 - MSWORD - Docx Filename - UTF-8''CHAPTER 3 MSWORDДокумент8 страницCHAPTER - 3 - MSWORD - Docx Filename - UTF-8''CHAPTER 3 MSWORDCaurrine MonsaludОценок пока нет
- CHAPTER - 3 - MSWORD - Do6cx Filename - UTF-8''CHAPTER 3 MSWORDДокумент8 страницCHAPTER - 3 - MSWORD - Do6cx Filename - UTF-8''CHAPTER 3 MSWORDCaurrine MonsaludОценок пока нет
- Classical PeriodДокумент4 страницыClassical PeriodCaurrine MonsaludОценок пока нет
- Brutas. ActivityДокумент14 страницBrutas. ActivityCaurrine MonsaludОценок пока нет
- It Caurrine MonsaludДокумент13 страницIt Caurrine MonsaludCaurrine MonsaludОценок пока нет
- Medication Scanning NRPДокумент12 страницMedication Scanning NRPapi-444018836Оценок пока нет
- Hiv ImradДокумент3 страницыHiv ImradKaren Mae Santiago AlcantaraОценок пока нет
- Nursing Concept Map TemplateДокумент4 страницыNursing Concept Map TemplateAris Kendell BungabongОценок пока нет
- Laporan Harian Pasien Puskesmas JatinegaraДокумент8 страницLaporan Harian Pasien Puskesmas JatinegaraanggaОценок пока нет
- AO CMFS During COVID-19Документ6 страницAO CMFS During COVID-19โสภาพรรณวดี รวีวารОценок пока нет
- Evidence 1.15.9-Change Log To Demonstrate The Differences Between 2017 and 2021 Edition PDFДокумент13 страницEvidence 1.15.9-Change Log To Demonstrate The Differences Between 2017 and 2021 Edition PDFKhalid ElwakilОценок пока нет
- Hemorragia Subaracnoidea AneurismaticaДокумент30 страницHemorragia Subaracnoidea AneurismaticajulianaОценок пока нет
- Neurogenic Shock Concept Map GuideДокумент1 страницаNeurogenic Shock Concept Map GuideJessa Mae Alforque Asentista0% (1)
- Under Guidance of Mr. Mali K.K. (Assistant Professor) : 1 Yspm, YtcДокумент41 страницаUnder Guidance of Mr. Mali K.K. (Assistant Professor) : 1 Yspm, YtcSabiruddin Mirza DipuОценок пока нет
- EEReview PDFДокумент7 страницEEReview PDFragavendharОценок пока нет
- NEET MDS 2021 Recall 151-200 Questions PDFДокумент183 страницыNEET MDS 2021 Recall 151-200 Questions PDFMahima Mishra100% (1)
- Study This Question Med Surg FinalДокумент14 страницStudy This Question Med Surg FinalAna Gonzalez83% (6)
- Lecture series explores issues in substance use disordersДокумент11 страницLecture series explores issues in substance use disordersRobyn AnОценок пока нет
- Community As Partner - Chapter 1Документ5 страницCommunity As Partner - Chapter 1KTОценок пока нет
- Pain Management JournalДокумент7 страницPain Management JournalPengurus Pusat HipgabiОценок пока нет
- The APN Professional Development Plan Paper - EditedДокумент8 страницThe APN Professional Development Plan Paper - Editedreginald wanyamaОценок пока нет
- Markel H - The Stethoscope and The Art of Listening 2006Документ3 страницыMarkel H - The Stethoscope and The Art of Listening 2006GeorgianaRamonaОценок пока нет
- Fingger Hold Exercises Relieve Joint Pain in ElderlyДокумент11 страницFingger Hold Exercises Relieve Joint Pain in Elderlyzakiyatul hikmahОценок пока нет
- Kajian Perilaku Kesehatan Dukun Terhadap Ibu Dan Bayi Setelah Melahirkan Suku Asli Dayak Meratus Kalimantan SelatanДокумент9 страницKajian Perilaku Kesehatan Dukun Terhadap Ibu Dan Bayi Setelah Melahirkan Suku Asli Dayak Meratus Kalimantan SelatanDIIIBID NISAОценок пока нет
- Mantoux TestДокумент3 страницыMantoux Testfarrukhhussain2006Оценок пока нет
- Hcml-Gms-Hse-Pn-Jsa-002 - Jsa (Rectification Pipeline GMS)Документ15 страницHcml-Gms-Hse-Pn-Jsa-002 - Jsa (Rectification Pipeline GMS)smk alirsyadyОценок пока нет
- China Oel Pil enДокумент2 страницыChina Oel Pil enmiksha100% (1)
- Sam PDFДокумент134 страницыSam PDFPunit Garg100% (2)
- Sujok Therapy FAQДокумент9 страницSujok Therapy FAQProbodh1100% (5)
- Helping Babies Breathe™ 06.27.2014Документ18 страницHelping Babies Breathe™ 06.27.2014Emily EresumaОценок пока нет
- Post Operative Care of PatientsДокумент37 страницPost Operative Care of Patientsapi-370869850% (2)
- Nursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleДокумент7 страницNursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleBridget Wilson100% (37)
- Health Status of Manitobans ReportДокумент78 страницHealth Status of Manitobans ReportCityNewsTorontoОценок пока нет
- Inversion of Uterus: By: Namita AryaДокумент29 страницInversion of Uterus: By: Namita Aryanamita0% (1)
- EthambutolДокумент1 страницаEthambutolSibel ErtuğrulОценок пока нет