Вам также может понравиться
- Kessler 2005Документ13 страницKessler 2005Web CrawlerОценок пока нет
- The Prevalence and Correlates of Adult ADHD in The United States - Results From The National Comorbidity Survey Replication PDFДокумент15 страницThe Prevalence and Correlates of Adult ADHD in The United States - Results From The National Comorbidity Survey Replication PDFRamoncito77Оценок пока нет
- Short Screening Scales To Monitor Population Prevalences and Trends in Non-Specific Psychological DistressДокумент18 страницShort Screening Scales To Monitor Population Prevalences and Trends in Non-Specific Psychological DistressDonald CabreraОценок пока нет
- Structure and Diagnosis of Adult Attention-Deficit/Hyperactivity DisorderДокумент11 страницStructure and Diagnosis of Adult Attention-Deficit/Hyperactivity DisordermavaddatasticОценок пока нет
- The Strengths and Difficulties Questionnaire: U.S. Normative Data and Psychometric PropertiesДокумент8 страницThe Strengths and Difficulties Questionnaire: U.S. Normative Data and Psychometric PropertiesIndra AjaОценок пока нет
- Prevalence, Persistence, and Sociodemographic Correlates of DSM-IV Disorders in The National Comorbidity Survey Replication Adolescent SupplementДокумент18 страницPrevalence, Persistence, and Sociodemographic Correlates of DSM-IV Disorders in The National Comorbidity Survey Replication Adolescent SupplementGaluh SabikhaОценок пока нет
- Yoa 40303Документ12 страницYoa 40303Dany MorBenОценок пока нет
- 16.new Adhd ParameterДокумент44 страницы16.new Adhd Parameterminha amoraОценок пока нет
- Prevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in The National Comorbidity Survey ReplicationДокумент11 страницPrevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in The National Comorbidity Survey ReplicationMuhammad NizarОценок пока нет
- Validity of The World Health Organization Adult ADHD Self-Report Scale (ASRS) Screener in A Representative Sample of Health Plan MembersДокумент14 страницValidity of The World Health Organization Adult ADHD Self-Report Scale (ASRS) Screener in A Representative Sample of Health Plan MembersCloudcynaraaОценок пока нет
- 1 s2.0 S0010440X15302169 MainДокумент4 страницы1 s2.0 S0010440X15302169 Mainlidia torres rosadoОценок пока нет
- 1 s2.0 S0890856709609552 MainДокумент9 страниц1 s2.0 S0890856709609552 Main서혜주Оценок пока нет
- 9/geriatric Depression Scale (GDS) : Clinical GerontologistДокумент10 страниц9/geriatric Depression Scale (GDS) : Clinical GerontologistTeresa GasparОценок пока нет
- CHAPTER 02, Literature ReviewДокумент27 страницCHAPTER 02, Literature ReviewAyesha ArshedОценок пока нет
- Hudziak 2004Документ9 страницHudziak 2004Alar Urrutikoetxea VicenteОценок пока нет
- A Study of Co-Morbidity in Mental RetardationДокумент9 страницA Study of Co-Morbidity in Mental RetardationijhrmimsОценок пока нет
- Comparing Various Short-Form Geriatric Depression Scales Leads To The GDS-5/15Документ5 страницComparing Various Short-Form Geriatric Depression Scales Leads To The GDS-5/15lucial86Оценок пока нет
- Accesare - Resursa 3Документ31 страницаAccesare - Resursa 3Rodica Pentea-PopОценок пока нет
- Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in The National Comorbidity Survey ReplicationДокумент11 страницLifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in The National Comorbidity Survey ReplicationCath-Kate LongОценок пока нет
- Article MSQOL-54Документ21 страницаArticle MSQOL-54bogdanneamtuОценок пока нет
- A New Clinical Scale For The Staging of DementiaДокумент8 страницA New Clinical Scale For The Staging of Dementiazitamugen.workОценок пока нет
- Psychometric Properties of The Hungarian Version oДокумент13 страницPsychometric Properties of The Hungarian Version oMohamed AbozeidОценок пока нет
- Anxiety Disorders Among Adolescents Referred To General Psychiatry For Multiple Causes: Clinical Presentation, Prevalence, and ComorbidityДокумент10 страницAnxiety Disorders Among Adolescents Referred To General Psychiatry For Multiple Causes: Clinical Presentation, Prevalence, and ComorbidityRatu CalistaОценок пока нет
- LiebowitzДокумент10 страницLiebowitzRalucaButaОценок пока нет
- KADSvs - BDIscreeningfordepression LeBlanc2002JChildAdolescPsychopharmДокумент16 страницKADSvs - BDIscreeningfordepression LeBlanc2002JChildAdolescPsychopharmRicardo ViolettiОценок пока нет
- Screening For Serious Mental Illness in The General PopulationДокумент6 страницScreening For Serious Mental Illness in The General PopulationDonald CabreraОценок пока нет
- Dementia in Medical StudentsДокумент1 страницаDementia in Medical StudentsAlexis RSОценок пока нет
- 08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsДокумент6 страниц08.06.09 - Psychosocial Impact of Dysthymia A Study Among Married PatientsRiham AmmarОценок пока нет
- Prevalence of Attention-De Ficit/ Hyperactivity Disorder: A Systematic Review and Meta-AnalysisДокумент10 страницPrevalence of Attention-De Ficit/ Hyperactivity Disorder: A Systematic Review and Meta-AnalysisDr Shobhit Kumar PrasadОценок пока нет
- Psychiatry Research: Review ArticleДокумент14 страницPsychiatry Research: Review Articlekhadidja BOUTOUILОценок пока нет
- 1.1 Buelens 2020Документ9 страниц1.1 Buelens 2020appaloosa.musicalОценок пока нет
- Evidence For The Reliability and Preliminary Validity of The Adult ADHD Self Report Scale v1.1 (ASRS v1.1) Screener in An Adolescent CommunityДокумент9 страницEvidence For The Reliability and Preliminary Validity of The Adult ADHD Self Report Scale v1.1 (ASRS v1.1) Screener in An Adolescent CommunityMeritxell PerezОценок пока нет
- Prevalence and Treatment of Mental Disorders Among US Children in The 2001-2004 NHANESДокумент9 страницPrevalence and Treatment of Mental Disorders Among US Children in The 2001-2004 NHANESDewi PrasetiaОценок пока нет
- Becke 2021Документ19 страницBecke 2021milord haalowen bombay wili laura4678Оценок пока нет
- Moffitt2015 PDFДокумент11 страницMoffitt2015 PDFRaul Morales VillegasОценок пока нет
- Brown (2001)Документ13 страницBrown (2001)Eunice_Pinto_1725Оценок пока нет
- RecommendedДокумент9 страницRecommendedMaya Putri Haryanti100% (1)
- ADHD For Children-AdolescentsДокумент28 страницADHD For Children-AdolescentsEdgar Prieto AmaralОценок пока нет
- Weitzman2004 PDFДокумент9 страницWeitzman2004 PDFDurga BalaОценок пока нет
- Volkert Et Al - 2018Документ7 страницVolkert Et Al - 2018dallaОценок пока нет
- JoHM 03 2018 ADHD KiGGS-Wave2Документ8 страницJoHM 03 2018 ADHD KiGGS-Wave2C AОценок пока нет
- Full TextДокумент10 страницFull Textammarashor78Оценок пока нет
- Norms For The Beck Depression Inventory (BDI-II) in A Large Dutch Community SampleДокумент6 страницNorms For The Beck Depression Inventory (BDI-II) in A Large Dutch Community SamplefanzefirlОценок пока нет
- Prevalence of ADD-ADHD in Older AdultsДокумент8 страницPrevalence of ADD-ADHD in Older AdultsRyan BОценок пока нет
- Mental HealthДокумент92 страницыMental HealthSAAD ALHALAFIОценок пока нет
- Management Guidelines For Anxiety Disorders in Children and AdolescentsДокумент23 страницыManagement Guidelines For Anxiety Disorders in Children and AdolescentsHari HaranОценок пока нет
- Hanley 2021Документ9 страницHanley 2021Web CrawlerОценок пока нет
- Screening For Adolescent Problem Drinking IdentificationADELE 1989Документ3 страницыScreening For Adolescent Problem Drinking IdentificationADELE 1989zgnrkfm4q9Оценок пока нет
- Clinical and Diagnostic Implications of Lifetime Attention-Deficit-Hyperactivity Disorder Comorbidity in Adults With Bipolar DisorderДокумент7 страницClinical and Diagnostic Implications of Lifetime Attention-Deficit-Hyperactivity Disorder Comorbidity in Adults With Bipolar DisorderCarla NapoliОценок пока нет
- JURNAL 1 Psychiatric Readmission of Children and Adolescents A Systematic Review and Meta-AnalysisДокумент11 страницJURNAL 1 Psychiatric Readmission of Children and Adolescents A Systematic Review and Meta-AnalysisNixal KurniawanОценок пока нет
- ADHD in Adults A Review of The LiteratureДокумент15 страницADHD in Adults A Review of The Literaturemeldovale100% (1)
- Michielsen 2013 - The Comorbidity of Anxiety and Depressive Symptoms in Older AdultsДокумент8 страницMichielsen 2013 - The Comorbidity of Anxiety and Depressive Symptoms in Older AdultsdaniellegarciaaaОценок пока нет
- A-Hudson, Hall & Harkness (2019)Документ11 страницA-Hudson, Hall & Harkness (2019)Jordanitha BhsОценок пока нет
- 2005 The Age-Dependent Decline of ADHD - A Meta-Analysis of Follow-Up StudiesДокумент7 страниц2005 The Age-Dependent Decline of ADHD - A Meta-Analysis of Follow-Up StudiesPiotr BuczkowiczОценок пока нет
- JSL 047Документ15 страницJSL 047Alí Jorkaeff Hernández LópezОценок пока нет
- Content ServerДокумент11 страницContent ServerTriismyОценок пока нет
- How Common Is Attention-Deficit/hyperactivity Disorder? Towards Resolution of The Controversy: Results From A Population-Based StudyДокумент5 страницHow Common Is Attention-Deficit/hyperactivity Disorder? Towards Resolution of The Controversy: Results From A Population-Based StudyDewi PrasetiaОценок пока нет
- New Research Posters: ResultsДокумент1 страницаNew Research Posters: ResultsKristoffer LoquiasОценок пока нет
- Prevalence of Attention-De Ficit/ Hyperactivity Disorder: A Systematic Review and Meta-AnalysisДокумент10 страницPrevalence of Attention-De Ficit/ Hyperactivity Disorder: A Systematic Review and Meta-AnalysisMalka SarmientoОценок пока нет
- Dimensional PsychopathologyОт EverandDimensional PsychopathologyMassimo BiondiОценок пока нет
- Towards Interactive Robots in Autism TherapyДокумент35 страницTowards Interactive Robots in Autism TherapyMihaela VișanОценок пока нет
- Ipol-Libe Et (2013) 474416 en PDFДокумент232 страницыIpol-Libe Et (2013) 474416 en PDFRobiОценок пока нет
- LIFEisGame Prototype - A Serious Game About Emotions For Children With AutismДокумент22 страницыLIFEisGame Prototype - A Serious Game About Emotions For Children With AutismMihaela VișanОценок пока нет
- Housing and Support Options For People With Autism FINAL PDFДокумент3 страницыHousing and Support Options For People With Autism FINAL PDFMihaela VișanОценок пока нет
- Progress Report On The Implementation of The European Disability Strategy (2010Документ200 страницProgress Report On The Implementation of The European Disability Strategy (2010Mihaela VișanОценок пока нет
- A Qualitative Study of Autism Policy in CanadaДокумент15 страницA Qualitative Study of Autism Policy in CanadaMihaela VișanОценок пока нет
- Autism - Overview of UK Policy and ServicesДокумент36 страницAutism - Overview of UK Policy and ServicesMihaela VișanОценок пока нет
- Guideline - Towards Inclusive Education For Children With Disabilities PDFДокумент162 страницыGuideline - Towards Inclusive Education For Children With Disabilities PDFMihaela VișanОценок пока нет
- Binge Eating Scale PDFДокумент3 страницыBinge Eating Scale PDFMihaela VișanОценок пока нет
- 2002 Scott Etal CASTДокумент39 страниц2002 Scott Etal CASTV_FreemanОценок пока нет
- Adult ADHD Self-Report Scale (ASRS) Symptom Checklist Adult ADHDДокумент4 страницыAdult ADHD Self-Report Scale (ASRS) Symptom Checklist Adult ADHDapi-12695071100% (12)
- Families With Disabled Children in Different European CountriesДокумент47 страницFamilies With Disabled Children in Different European CountriesMihaela VișanОценок пока нет
- 6question ADHD ASRS v1 1 PDFДокумент3 страницы6question ADHD ASRS v1 1 PDFMihaela VișanОценок пока нет
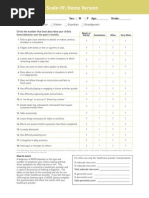
- Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom ChecklistДокумент2 страницыAdult ADHD Self-Report Scale (ASRS-v1.1) Symptom ChecklistMihaela VișanОценок пока нет
- Criterii DG Scleroza Tuberoasa 2012Документ12 страницCriterii DG Scleroza Tuberoasa 2012Mihaela VișanОценок пока нет
- Eligibility Criteria FP 2016 FinalДокумент1 страницаEligibility Criteria FP 2016 FinalAndreea LaviniaОценок пока нет
- DIVA - 2 - EN - FORM - Invulbaar PDFДокумент20 страницDIVA - 2 - EN - FORM - Invulbaar PDFGerencia Publimax100% (1)
- Score of Inattention Subscale of ADHD Rating Scale-IV Is Significantly Higher For AD/HD Than PDDДокумент6 страницScore of Inattention Subscale of ADHD Rating Scale-IV Is Significantly Higher For AD/HD Than PDDMihaela VișanОценок пока нет
- Screening ADHDДокумент2 страницыScreening ADHDPsiholog Alina Mirela CraiuОценок пока нет
- A Clinical Approach To The Diagnosis of Patients With Leukodystrophies and Genetic LeukoencephelopathiesДокумент29 страницA Clinical Approach To The Diagnosis of Patients With Leukodystrophies and Genetic LeukoencephelopathiesMihaela VișanОценок пока нет
- MidodrineДокумент2 страницыMidodrineMihaela VișanОценок пока нет
- OxaliplatinДокумент3 страницыOxaliplatinMihaela VișanОценок пока нет
- VGF or VGF Nerve Growth Factor Inducible Is A Protein and Neuropeptide That May Play A Role in Regulating Energy HomeostasisДокумент1 страницаVGF or VGF Nerve Growth Factor Inducible Is A Protein and Neuropeptide That May Play A Role in Regulating Energy HomeostasisMihaela VișanОценок пока нет
- Angio DysplasiaДокумент2 страницыAngio DysplasiaMihaela VișanОценок пока нет
- The RectumДокумент4 страницыThe RectumMihaela VișanОценок пока нет
- OctreotideДокумент4 страницыOctreotideMihaela VișanОценок пока нет
- The Large IntestineДокумент9 страницThe Large IntestineMihaela VișanОценок пока нет
- HepatitisДокумент10 страницHepatitisMihaela VișanОценок пока нет
- Final MicrobiologiaaaaДокумент199 страницFinal MicrobiologiaaaaMartin RodriguezОценок пока нет
- Field Security Manual Section 1-6Документ37 страницField Security Manual Section 1-6eugenia100% (2)
- Payslip Payslip Employee Name: Employee Name: Deparment DeparmentДокумент22 страницыPayslip Payslip Employee Name: Employee Name: Deparment DeparmentSharlin OrolaОценок пока нет
- pdf14 - Bioabfv - Engl - BFДокумент94 страницыpdf14 - Bioabfv - Engl - BFEdu FrancoОценок пока нет
- QUALI 2016 Coping Strategies of Taiwanese Children With ASDДокумент14 страницQUALI 2016 Coping Strategies of Taiwanese Children With ASDezaОценок пока нет
- DAFTAR PUSTAKA HydrocephalusДокумент2 страницыDAFTAR PUSTAKA HydrocephalusRahma darisОценок пока нет
- Health Declaration Form A1 Whole PageДокумент1 страницаHealth Declaration Form A1 Whole PageFedelyn SemenianoОценок пока нет
- Micro Paper On Unknown BacteriaДокумент10 страницMicro Paper On Unknown BacteriaPedro Alonso Titi Benavente100% (1)
- Narcissism - Gral Def - 1 of TH 3 Triadic Dark Perosnality Traits With Psychopathy & Machiavellism - Wi EN 17sep2014Документ23 страницыNarcissism - Gral Def - 1 of TH 3 Triadic Dark Perosnality Traits With Psychopathy & Machiavellism - Wi EN 17sep2014jffm7147Оценок пока нет
- Child Psychology Psychiatry - 2020 - Lavis - Online Harms or Benefits An Ethnographic Analysis of The Positives andДокумент13 страницChild Psychology Psychiatry - 2020 - Lavis - Online Harms or Benefits An Ethnographic Analysis of The Positives andclaudyaОценок пока нет
- New Principles in Pilon Fractres ManagementДокумент17 страницNew Principles in Pilon Fractres ManagementCamila FontechaОценок пока нет
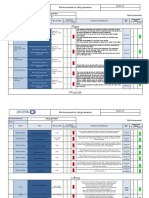
- Plant 6 3: Risk Assessment For Lifting OperationsДокумент4 страницыPlant 6 3: Risk Assessment For Lifting OperationsIdris AdeniranОценок пока нет
- PPP - Reading B - Test 3 Question PaperДокумент6 страницPPP - Reading B - Test 3 Question PaperLina CornickОценок пока нет
- MChiro Prospectus 2021Документ22 страницыMChiro Prospectus 2021Aura-Elena BugusОценок пока нет
- Physiological Responses To Lead Exposure in Wheat, Barley and OatДокумент6 страницPhysiological Responses To Lead Exposure in Wheat, Barley and OatVince RomanoОценок пока нет
- O Slide Method - Most Commonly Used o Cover Glass Method o Spin MethodДокумент5 страницO Slide Method - Most Commonly Used o Cover Glass Method o Spin MethodAngela ReyesОценок пока нет
- The Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of AsiaДокумент28 страницThe Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of Asiaojay_88Оценок пока нет
- Excessive Alcohol UseДокумент1 страницаExcessive Alcohol UseABC10Оценок пока нет
- Chapter 1 & 2 PDFДокумент15 страницChapter 1 & 2 PDF11D3 CHUA , Jasmine B.Оценок пока нет
- Managing and Caring For The SelfДокумент17 страницManaging and Caring For The SelfYen Yen100% (1)
- Health Law First DraftДокумент10 страницHealth Law First DraftNAYAN SINGHОценок пока нет
- MADE EASY PublicationsДокумент10 страницMADE EASY PublicationsSaket PandeyОценок пока нет
- Safety Data Sheet: 1. IdentificationДокумент5 страницSafety Data Sheet: 1. IdentificationOmar SaaedОценок пока нет
- Intervention Approaches Table 8 - 3 Edition: Create, PromoteДокумент1 страницаIntervention Approaches Table 8 - 3 Edition: Create, PromoteJM RMОценок пока нет
- You're Already: Le M Ge o M KneeДокумент3 страницыYou're Already: Le M Ge o M KneeSara CoonОценок пока нет
- Current Transcriber Test TextДокумент1 страницаCurrent Transcriber Test TextTalking Cats PlaytimeОценок пока нет
- Practical Research 2Документ7 страницPractical Research 2Jesa mae TorinoОценок пока нет
- Bioethics Session 16 SASДокумент4 страницыBioethics Session 16 SASAnthony BadiliОценок пока нет
- Positioning and Its ImportanceДокумент22 страницыPositioning and Its ImportanceDeepika PatidarОценок пока нет
- Journal On Self ConceptДокумент6 страницJournal On Self Conceptkspsridharan4899Оценок пока нет