Вам также может понравиться
- Neuropsychological Tests & Cognitive ImpairmentДокумент8 страницNeuropsychological Tests & Cognitive ImpairmentKaycee JLОценок пока нет
- DementiaДокумент35 страницDementiaalishba iqbal 1112Оценок пока нет
- Table 59-5 - Clinical Features of Common DementiasДокумент1 страницаTable 59-5 - Clinical Features of Common DementiasDragutin PetrićОценок пока нет
- Dementia 2Документ51 страницаDementia 2Arsal MushtaqОценок пока нет
- Diagrams & Illustrations of Dementia Signs & SymptomsДокумент1 страницаDiagrams & Illustrations of Dementia Signs & Symptomsdysa ayu shalsabilaОценок пока нет
- Physical development in early adulthoodДокумент3 страницыPhysical development in early adulthoodSATOR DOMINICОценок пока нет
- Alzheimers DiseaseДокумент1 страницаAlzheimers DiseaseMartha Marty BalintОценок пока нет
- What, Where, & How Systems Agnosias!Документ28 страницWhat, Where, & How Systems Agnosias!Asma ShahОценок пока нет
- Neurocognitive Disorder Diagnosis and TreatmentДокумент3 страницыNeurocognitive Disorder Diagnosis and TreatmentIT’S ME HAYLAОценок пока нет
- 36 Applied NeuroscienceДокумент26 страниц36 Applied Neurosciencecercuri pătrate de fumОценок пока нет
- After The Diagnosis: Rehabilitation & Support Options For Mild DementiaДокумент31 страницаAfter The Diagnosis: Rehabilitation & Support Options For Mild DementiaDivya pathakОценок пока нет
- Neuro Behavior DisordersДокумент80 страницNeuro Behavior Disordersmohamadafif_drОценок пока нет
- Seminar DementiaДокумент63 страницыSeminar DementiaAhmad Syahmi YZОценок пока нет
- Understanding the brain and common cognitive impairmentsДокумент5 страницUnderstanding the brain and common cognitive impairmentsAkash KОценок пока нет
- Amnesia DemensiaДокумент2 страницыAmnesia DemensiaAlexander TegarОценок пока нет
- Strategies at A GlanceДокумент13 страницStrategies at A Glanceapi-483842715Оценок пока нет
- DementiaДокумент43 страницыDementiaMelkamu TulbakeОценок пока нет
- Care of Older Adults (Finals)Документ14 страницCare of Older Adults (Finals)Ax’l SisterОценок пока нет
- Osmosis 1Документ1 страницаOsmosis 1dysa ayu shalsabilaОценок пока нет
- Delirium, Dementia & Amnestic Cognitive DisordersДокумент33 страницыDelirium, Dementia & Amnestic Cognitive Disordersapi-369624875% (4)
- Alzheimer's Disease: DementiaДокумент18 страницAlzheimer's Disease: DementiaBerny VillavicencioОценок пока нет
- Major & Mild NCD Terminology UpdatesДокумент30 страницMajor & Mild NCD Terminology Updatesrachelle anne merallesОценок пока нет
- 0 S12 Cognition Dementia 1111 20 BBДокумент81 страница0 S12 Cognition Dementia 1111 20 BBMichael MerlinОценок пока нет
- Dementia PDFДокумент19 страницDementia PDFANGELA ERES BALINGBINGОценок пока нет
- CBD Team e PsychiatryДокумент44 страницыCBD Team e PsychiatrydindanovitamОценок пока нет
- Rehabilitasi Medis Untuk GSA - Dr. LuhДокумент32 страницыRehabilitasi Medis Untuk GSA - Dr. LuhDoc HadiОценок пока нет
- Fact Sheet - Brain Map and FunctionsДокумент4 страницыFact Sheet - Brain Map and FunctionsAbdualaziz AlmalkiОценок пока нет
- Care of The Older AdultsДокумент17 страницCare of The Older AdultsL Rean Carmelle MAGALLONESОценок пока нет
- 117 Delirium and DementiaДокумент6 страниц117 Delirium and DementiaLa VicОценок пока нет
- Neuro ScienceДокумент36 страницNeuro ScienceSHAMBHAVI MISHRAОценок пока нет
- The Minimally Conscious State: Definition and Diagnostic CriteriaДокумент7 страницThe Minimally Conscious State: Definition and Diagnostic CriteriadonnyawОценок пока нет
- ALZHEIMERДокумент2 страницыALZHEIMERLorelyn Santos CorpuzОценок пока нет
- Dementias Claudia & AndreaДокумент11 страницDementias Claudia & AndreaandreafalanganunezОценок пока нет
- Week 4 NotesДокумент27 страницWeek 4 NotesRayОценок пока нет
- Disabilit Y: An Effort By:-Sehaj Saubhagya PriyamДокумент14 страницDisabilit Y: An Effort By:-Sehaj Saubhagya PriyamSehaj SinghОценок пока нет
- 5-Minute Screening Neurologic ExamДокумент27 страниц5-Minute Screening Neurologic ExamshafijanОценок пока нет
- Differentiating The Dementias: A Neurological Approach: ReviewДокумент8 страницDifferentiating The Dementias: A Neurological Approach: ReviewJemellee CanoОценок пока нет
- PSYCHIATRIC NURSING AnjaliДокумент47 страницPSYCHIATRIC NURSING AnjaliAnjali GuptaОценок пока нет
- Components of Mental Status ExaminationДокумент5 страницComponents of Mental Status ExaminationDesta FransiscaОценок пока нет
- Behavior and Mental StatusДокумент41 страницаBehavior and Mental StatusGokul Poudel100% (1)
- Sensory Based Intervention For InternsДокумент80 страницSensory Based Intervention For InternsStratiatella Faith AnthonyОценок пока нет
- Dissociative Disorders and Personality Disorders NotesДокумент6 страницDissociative Disorders and Personality Disorders NoteselaineОценок пока нет
- Nursing Neurology Part 1Документ26 страницNursing Neurology Part 1tina.flores16Оценок пока нет
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaДокумент62 страницыAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2Оценок пока нет
- Visuoperceptual Difficulties in DementiaДокумент8 страницVisuoperceptual Difficulties in DementiaLoz RamseyОценок пока нет
- Mental Status ExaminationДокумент72 страницыMental Status Examinationsherief marouf100% (1)
- Right Hemisphere DamageДокумент80 страницRight Hemisphere DamageSweekriti Narayanan100% (2)
- Neurological AssessmentДокумент10 страницNeurological AssessmentmatsumotoОценок пока нет
- 08.06 Abnormal Psychology-Revised NotesДокумент6 страниц08.06 Abnormal Psychology-Revised NotesJesusa Angelika IlustreОценок пока нет
- Pe NotesДокумент20 страницPe NotesHim SharОценок пока нет
- Dementia & DeliriumДокумент7 страницDementia & DeliriumSudesna Roy ChowdhuryОценок пока нет
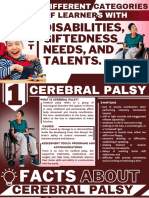
- Different Learning Needs and AbilitiesДокумент22 страницыDifferent Learning Needs and AbilitiesMichael John Paul EspejonОценок пока нет
- Exam FlashcardsДокумент115 страницExam FlashcardsOT PRACTICE TIMEОценок пока нет
- NURSING 21 Sensory PerceptionДокумент2 страницыNURSING 21 Sensory PerceptionKareen SornitoОценок пока нет
- Table of DementiaДокумент3 страницыTable of DementiaCrystal GaoОценок пока нет
- Rehab IST_CVIДокумент31 страницаRehab IST_CVIashleighmarshall05Оценок пока нет
- Lewy Body Dementia: Causes, Tests and Treatment OptionsОт EverandLewy Body Dementia: Causes, Tests and Treatment OptionsРейтинг: 4 из 5 звезд4/5 (1)
- Accelerated Learning and Unlimited Memory Techniques and Strategies: Real Coaching from a Real Expert. Tips & Tricks for Students and AdultsОт EverandAccelerated Learning and Unlimited Memory Techniques and Strategies: Real Coaching from a Real Expert. Tips & Tricks for Students and AdultsРейтинг: 4 из 5 звезд4/5 (2)
- Frailty: Geriatrics Evaluation & ManagementДокумент2 страницыFrailty: Geriatrics Evaluation & ManagementAngeles SlzrОценок пока нет
- Diabetes Mellitus: Geriatrics Evaluation & ManagementДокумент4 страницыDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrОценок пока нет
- Depression: Geriatrics Evaluation & ManagementДокумент2 страницыDepression: Geriatrics Evaluation & ManagementAngeles SlzrОценок пока нет
- Delirium: Geriatrics Evaluation & ManagementДокумент2 страницыDelirium: Geriatrics Evaluation & ManagementFer MacОценок пока нет
- Hola MundoДокумент1 страницаHola MundoAngeles SlzrОценок пока нет
- Hola MundoДокумент1 страницаHola MundoAngeles SlzrОценок пока нет
- Fee Shedule 2020-21 Final DiosДокумент2 страницыFee Shedule 2020-21 Final Diosapi-210356903Оценок пока нет
- Pitagan discusses media, eLearning, 21st century learningДокумент34 страницыPitagan discusses media, eLearning, 21st century learningReymond CuisonОценок пока нет
- A Reaction Paper On Russell's Is Happiness Still PossibleДокумент4 страницыA Reaction Paper On Russell's Is Happiness Still PossibleElizier 'Barlee' B. LazoОценок пока нет
- Annotated BibliographyДокумент3 страницыAnnotated Bibliographyapi-406951522Оценок пока нет
- Goshgar Narimanli: Work ExperienceДокумент2 страницыGoshgar Narimanli: Work ExperienceZiyaОценок пока нет
- Evan Kegler: 5280 Coquina Key DR SE, St. Petersburg, FL Ekegler@law - Stetson.edu - 352-422-1396Документ1 страницаEvan Kegler: 5280 Coquina Key DR SE, St. Petersburg, FL Ekegler@law - Stetson.edu - 352-422-1396api-306719857Оценок пока нет
- Academic Resources Worksheet Maya TraceyДокумент1 страницаAcademic Resources Worksheet Maya Traceyapi-340525387Оценок пока нет
- Manasi Patil - Why Read Shakespeare Complete Text Embedded Work MasterДокумент8 страницManasi Patil - Why Read Shakespeare Complete Text Embedded Work Masterapi-3612704670% (1)
- Transcendentalism EssayДокумент4 страницыTranscendentalism Essayapi-248448724Оценок пока нет
- HBET1303Документ216 страницHBET1303Tce ShikinОценок пока нет
- Written Output For Title DefenseДокумент6 страницWritten Output For Title DefensebryanОценок пока нет
- Hbet 4603 AssignmentsДокумент13 страницHbet 4603 Assignmentschristina lawieОценок пока нет
- BCPC ResolutionДокумент2 страницыBCPC ResolutionSamuel CastroОценок пока нет
- Face Recognition Based Attendance SystemДокумент9 страницFace Recognition Based Attendance SystemIJRASETPublicationsОценок пока нет
- AssignmentДокумент3 страницыAssignmentNeha Singhal50% (2)
- Alvar Aalto 1Документ4 страницыAlvar Aalto 1Santiago Martínez GómezОценок пока нет
- Globalization's Impact on Education SystemsДокумент25 страницGlobalization's Impact on Education SystemsCJ Castro100% (1)
- ML in DBS Systematic Review PreprintДокумент20 страницML in DBS Systematic Review PreprintBen AllenОценок пока нет
- Comparative Education AustraliaДокумент2 страницыComparative Education AustraliaJoseph Eric Nardo100% (1)
- Demonstration FormДокумент2 страницыDemonstration FormDomric Panunciar100% (1)
- Child and Adolescent DevelopmentДокумент5 страницChild and Adolescent Developmentandrew gauranaОценок пока нет
- FORM SSC.1 School Sports Club Registration Form v1 SMAДокумент3 страницыFORM SSC.1 School Sports Club Registration Form v1 SMABaluyut Edgar Jr. MОценок пока нет
- Abigail Pelletier Teaching ResumeДокумент4 страницыAbigail Pelletier Teaching Resumeapi-253261843Оценок пока нет
- Department of Education: Classroom Readiness ChecklistДокумент3 страницыDepartment of Education: Classroom Readiness ChecklistL.V. BendañaОценок пока нет
- 3D Terrain Car Racing GameДокумент38 страниц3D Terrain Car Racing Gamerao sbОценок пока нет
- PDNE With PDLNE PDFДокумент46 страницPDNE With PDLNE PDFJamshihas ApОценок пока нет
- Emotional Intelligence: Anuj JindalДокумент19 страницEmotional Intelligence: Anuj JindalSpoorthi MeruguОценок пока нет
- Manage Software ProjectsДокумент4 страницыManage Software ProjectsRas Abel BekeleОценок пока нет
- Directed Writing NotesДокумент3 страницыDirected Writing Notesnasha yacob75% (4)
- EEE513 Nanophotonics Current SyllabusДокумент2 страницыEEE513 Nanophotonics Current Syllabusdineshshan100% (1)