Вам также может понравиться
- The Anatomy of the Horse's Foot and Hoof - A Collection of Historical Articles on the Physiology and Function of the Foot and HoofОт EverandThe Anatomy of the Horse's Foot and Hoof - A Collection of Historical Articles on the Physiology and Function of the Foot and HoofОценок пока нет
- 18 MSK Arm and HandДокумент27 страниц18 MSK Arm and HandNTRisforthinkersОценок пока нет
- Osteology of Upper LimbДокумент13 страницOsteology of Upper Limbdie1only100% (1)
- Knee Anatomy Osseous Structures: Concept InformationДокумент19 страницKnee Anatomy Osseous Structures: Concept InformationRachel BlackburnОценок пока нет
- Knee Joint Anatomy ManualДокумент6 страницKnee Joint Anatomy ManualDungani AllanОценок пока нет
- Anatomi AnkleДокумент15 страницAnatomi AnkleZera DirgantaraОценок пока нет
- Norm Anatomy Elbow 2011Документ11 страницNorm Anatomy Elbow 2011Екатерина БербецОценок пока нет
- Knee Complex: 1: BiomechanicsДокумент33 страницыKnee Complex: 1: BiomechanicsMichael SelvarajОценок пока нет
- Biomechanics of The Human SpineДокумент5 страницBiomechanics of The Human SpineLusian VissОценок пока нет
- Solomon Ankle Injury PDFДокумент9 страницSolomon Ankle Injury PDFHikmah Wahid AkbarОценок пока нет
- Anatomy of The Ankle and FootДокумент13 страницAnatomy of The Ankle and FootRichard MillerОценок пока нет
- Snell Lower LimbДокумент44 страницыSnell Lower LimbBen100% (3)
- Anatomia y Biomecanica Pie TobilloДокумент21 страницаAnatomia y Biomecanica Pie TobilloJoel OntiverosОценок пока нет
- Bones of The Upper LimbДокумент46 страницBones of The Upper LimbSoze KeyserОценок пока нет
- Spine Biomechanics: Mer/Bio Soft Tissue Mechanics SB-1Документ11 страницSpine Biomechanics: Mer/Bio Soft Tissue Mechanics SB-1Sarah Magdy100% (1)
- Acetabular LabrumДокумент31 страницаAcetabular LabrumhaminatrafОценок пока нет
- StructureДокумент7 страницStructureNeirfla WassabiОценок пока нет
- Anatomy Summary BasicДокумент54 страницыAnatomy Summary BasicDungani AllanОценок пока нет
- 36 Reading RapoffДокумент11 страниц36 Reading RapoffFanica ScarlatОценок пока нет
- B1fe PDFДокумент13 страницB1fe PDFKiki Apdillah FeriОценок пока нет
- Anatomy, Shoulder and Upper Limb, Clavicle - StatPearls - NCBI BookshelfДокумент7 страницAnatomy, Shoulder and Upper Limb, Clavicle - StatPearls - NCBI BookshelfRizqan Fahlevvi AkbarОценок пока нет
- Lumbarization of First Sacral VertebraДокумент4 страницыLumbarization of First Sacral VertebraangellisimalОценок пока нет
- Vertebra: StructureДокумент9 страницVertebra: StructureayudhyaОценок пока нет
- L12Документ45 страницL12Ahmed El goharyОценок пока нет
- Anatomy of The Pelvis (Pelvic Ring)Документ17 страницAnatomy of The Pelvis (Pelvic Ring)Iskolar MorenoОценок пока нет
- 3 Functional Anatomy of The Knee: D. G. EckhoffДокумент7 страниц3 Functional Anatomy of The Knee: D. G. EckhoffCiberОценок пока нет
- Naik, S. - Biomechanics of Knee ComplexДокумент25 страницNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- Definition of Shoulder DislocationДокумент66 страницDefinition of Shoulder DislocationDeepika verma100% (1)
- Tecklenburg 2005Документ6 страницTecklenburg 2005GERARDO TORRES RUIZОценок пока нет
- ST - Paulos Hospital Millennium Medical College: Gross Anatomy:Upper LimbДокумент256 страницST - Paulos Hospital Millennium Medical College: Gross Anatomy:Upper LimbetОценок пока нет
- Anatomy and Physiology of The Hip BoneДокумент8 страницAnatomy and Physiology of The Hip BoneBeGie MamBaОценок пока нет
- Gross Anatomy I OsteologyДокумент42 страницыGross Anatomy I OsteologySonia FelixОценок пока нет
- Neurobiomecanica de PelvisДокумент34 страницыNeurobiomecanica de PelvisPaula Bustamante MuñozОценок пока нет
- Subtalar Joint Instability: Current Clinical Concepts: Adam Budny, DPMДокумент12 страницSubtalar Joint Instability: Current Clinical Concepts: Adam Budny, DPMAnonymous kdBDppigEОценок пока нет
- Oseo UppДокумент28 страницOseo UppMariana Mojica DiazОценок пока нет
- BooksДокумент388 страницBooksMayank GoyalОценок пока нет
- Coxae), Is The Joint Between The Femur and Acetabulum of The Pelvis and ItsДокумент9 страницCoxae), Is The Joint Between The Femur and Acetabulum of The Pelvis and ItsHLОценок пока нет
- Fulltext - Smjca v2 1015Документ8 страницFulltext - Smjca v2 1015Chis AlexandraОценок пока нет
- Anatomy and PhysiologyДокумент4 страницыAnatomy and PhysiologySarah CabalquintoОценок пока нет
- The Hip JointДокумент4 страницыThe Hip Jointshash82Оценок пока нет
- AD 5 Vertebral AnatomyДокумент37 страницAD 5 Vertebral AnatomyLintang ZerlinaОценок пока нет
- Ankle & Foot MechanicsДокумент47 страницAnkle & Foot MechanicsAhmed El goharyОценок пока нет
- Functional Anatomy of The SpineДокумент14 страницFunctional Anatomy of The SpinebandiiitzОценок пока нет
- The Anterolateral Complex of The Knee: A Pictorial EssayДокумент6 страницThe Anterolateral Complex of The Knee: A Pictorial EssayLISETTE TRICIA MALIPEROОценок пока нет
- Bio-Mechanics of Ankle-Foot JointДокумент70 страницBio-Mechanics of Ankle-Foot JointIipo ChennaiОценок пока нет
- List BonesДокумент38 страницList Bonesshahera rosdiОценок пока нет
- ClavicleДокумент9 страницClavicleMarshmalloowОценок пока нет
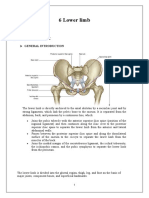
- 6 Lower LimbДокумент19 страниц6 Lower LimbMOHAMMED BIN BAREKОценок пока нет
- Bryce2008 PDFДокумент14 страницBryce2008 PDFsoylahijadeunvampiroОценок пока нет
- Ankle N Foot 1&2Документ54 страницыAnkle N Foot 1&2YusraОценок пока нет
- Anatomy and Physiology of The SpineДокумент12 страницAnatomy and Physiology of The SpineKinahZildredBibitОценок пока нет
- Blount's Disease (Textbook)Документ17 страницBlount's Disease (Textbook)Fadzhil AmranОценок пока нет
- Lectura Previ2 - U1-M6-T4-CAPITULO LESIONES DE PIE 2Документ13 страницLectura Previ2 - U1-M6-T4-CAPITULO LESIONES DE PIE 2Maria De Los Angeles Vitteri EdenОценок пока нет
- The Skeletal System: The Appendicular SkeletonДокумент43 страницыThe Skeletal System: The Appendicular Skeletonjonas hingcoОценок пока нет
- Anatomic Moment: Optic Canal Forms An Angle of AboutДокумент7 страницAnatomic Moment: Optic Canal Forms An Angle of AboutJennifer RodriguezОценок пока нет
- Blount's Disease (Textbook)Документ17 страницBlount's Disease (Textbook)Fadzhil AmranОценок пока нет
- Abjs 8 332Документ11 страницAbjs 8 332angelluis1980Оценок пока нет
- College of Human Sciences & Psychology Department: ClavicleДокумент17 страницCollege of Human Sciences & Psychology Department: ClavicleJohn Patrick LagmayОценок пока нет
- 8 The Appendicular Skeleton: Chapter ObjectivesДокумент48 страниц8 The Appendicular Skeleton: Chapter ObjectivessinnueОценок пока нет
- A) Hallux Adductor o Abductor Muscle PDFДокумент2 страницыA) Hallux Adductor o Abductor Muscle PDFericdgОценок пока нет
- Diabetic Foot Ulcers A ReviewДокумент14 страницDiabetic Foot Ulcers A ReviewEduardo FrancoОценок пока нет
- A) The Course of The Super Cial Peroneal Nerve in Relation To The Ankle Position. Anatomical Study With Ankle Arthroscopic Implications PDFДокумент6 страницA) The Course of The Super Cial Peroneal Nerve in Relation To The Ankle Position. Anatomical Study With Ankle Arthroscopic Implications PDFericdgОценок пока нет
- Role of Food-Derived Antioxidant Agents Against Acetaminophen-Induced HepatotoxicityДокумент14 страницRole of Food-Derived Antioxidant Agents Against Acetaminophen-Induced HepatotoxicityericdgОценок пока нет
- A) Biphalangeal Fifth Toe PDFДокумент4 страницыA) Biphalangeal Fifth Toe PDFericdgОценок пока нет
- A) The Anatomy in Relation To Injury of The Lateral Collateral Ligaments of The Ankle PDFДокумент8 страницA) The Anatomy in Relation To Injury of The Lateral Collateral Ligaments of The Ankle PDFericdgОценок пока нет
- Pain Management For Elective Foot and Ankle Surgery. A Systematic Review of Randomized Controlled Trials PDFДокумент11 страницPain Management For Elective Foot and Ankle Surgery. A Systematic Review of Randomized Controlled Trials PDFericdgОценок пока нет
- Varidase. The Science Behind The Medicament PDFДокумент4 страницыVaridase. The Science Behind The Medicament PDFericdgОценок пока нет
- Ankle Anatomy LigamentsДокумент13 страницAnkle Anatomy LigamentsKaren Torres PantojaОценок пока нет
- Pain Management For Elective Foot and Ankle Surgery. A Systematic Review of Randomized Controlled Trials PDFДокумент11 страницPain Management For Elective Foot and Ankle Surgery. A Systematic Review of Randomized Controlled Trials PDFericdgОценок пока нет
- A) Anatomy and Physiology of The Extensor Apparatus of The Toes PDFДокумент12 страницA) Anatomy and Physiology of The Extensor Apparatus of The Toes PDFericdgОценок пока нет
- Literatur AДокумент1 страницаLiteratur AericdgОценок пока нет
- Varidase. The Science Behind The Medicament PDFДокумент4 страницыVaridase. The Science Behind The Medicament PDFericdgОценок пока нет
- Varidase. The Science Behind The Medicament PDFДокумент4 страницыVaridase. The Science Behind The Medicament PDFericdgОценок пока нет
- DFFFFGGGДокумент1 страницаDFFFFGGGericdgОценок пока нет
- RRRGДокумент1 страницаRRRGericdgОценок пока нет
- Randall Selitto TestДокумент1 страницаRandall Selitto TestericdgОценок пока нет
- DDDДокумент1 страницаDDDericdgОценок пока нет
- RRRGДокумент1 страницаRRRGericdgОценок пока нет
- RGGGGGДокумент1 страницаRGGGGGericdgОценок пока нет
- DofdeeeДокумент1 страницаDofdeeeericdgОценок пока нет
- RRRRRRRRДокумент1 страницаRRRRRRRRericdgОценок пока нет
- HerowieffДокумент1 страницаHerowieffericdgОценок пока нет
- HGRQДокумент1 страницаHGRQericdgОценок пока нет
- Installation, Operation, and Maintenance Manual: Model Ic I-Frame, Ici I-Frame, Ich I-Frame, Icih I-FrameДокумент76 страницInstallation, Operation, and Maintenance Manual: Model Ic I-Frame, Ici I-Frame, Ich I-Frame, Icih I-FrameJOSE GARCIAОценок пока нет
- Brother Sewing Machine Operation ManualДокумент52 страницыBrother Sewing Machine Operation ManualSarahFalk100% (1)
- Syncope ShockДокумент39 страницSyncope ShockBunga Erlita RosaliaОценок пока нет
- People v. Dalag y Custodio 402 SCRA 254 PDFДокумент27 страницPeople v. Dalag y Custodio 402 SCRA 254 PDFfelix camerinoОценок пока нет
- Structured Teaching Programme On Basic Life Support in Paediatric EmergenciesДокумент18 страницStructured Teaching Programme On Basic Life Support in Paediatric EmergenciesBalkrishn SarswatОценок пока нет
- YogaДокумент34 страницыYogaVarsha KrishnanОценок пока нет
- Activity#1Документ2 страницыActivity#1LINDA RAGUINDINОценок пока нет
- Cat Vs Dog Anatomy Anatomical DifferencesДокумент2 страницыCat Vs Dog Anatomy Anatomical DifferencesAlliОценок пока нет
- Extensor Tendon Injury ProtocolДокумент11 страницExtensor Tendon Injury ProtocoltasneempichoriОценок пока нет
- Orthopedic NursingДокумент21 страницаOrthopedic NursingCris Constantino San JuanОценок пока нет
- Risk Assessment Template For Fit-OutДокумент5 страницRisk Assessment Template For Fit-OutJedz Gumapas79% (14)
- Parade 2 Februari 2023 Tanpa AsaДокумент25 страницParade 2 Februari 2023 Tanpa Asaputra syawalОценок пока нет
- The Bricklayer's Accident ReportДокумент1 страницаThe Bricklayer's Accident ReportSara FontanОценок пока нет
- Nnadili v. Chevron U.s.a., Inc.Документ10 страницNnadili v. Chevron U.s.a., Inc.RavenFoxОценок пока нет
- Chest Trauma and Diseases: Mexigin Gayatri Akash JohannaДокумент80 страницChest Trauma and Diseases: Mexigin Gayatri Akash JohannadidiОценок пока нет
- Jurnal AntibiotikДокумент5 страницJurnal AntibiotikSela PutrianaОценок пока нет
- Hazard Analysis and Risk Assessment (HARA)Документ31 страницаHazard Analysis and Risk Assessment (HARA)Sauvik ChakrabortyОценок пока нет
- Aseptic TechniquesДокумент21 страницаAseptic TechniquesSarah Eddiah100% (1)
- Accident Mannual (English) 1 PDFДокумент295 страницAccident Mannual (English) 1 PDFPoonamKumariSahaОценок пока нет
- NCLEX - Review (6514)Документ51 страницаNCLEX - Review (6514)whereswaldo007yahooc100% (1)
- Central Post-Stroke Pain - Clinical Characteristics, Pathophysiology, and ManagementДокумент12 страницCentral Post-Stroke Pain - Clinical Characteristics, Pathophysiology, and ManagementKarimah Ihda Husna YainОценок пока нет
- Diagnosis and Management of Piriformis SyndromeДокумент4 страницыDiagnosis and Management of Piriformis Syndromearie ikaОценок пока нет
- Shoulder Pain - The Supraspinatous MuscleДокумент6 страницShoulder Pain - The Supraspinatous Musclesale18100% (1)
- Group 2 TleДокумент40 страницGroup 2 Tleralph divinaОценок пока нет
- Cerebral Protection & NeuroresuscitationДокумент19 страницCerebral Protection & NeuroresuscitationImad El SadekОценок пока нет
- Coaching PortfolioДокумент74 страницыCoaching Portfolioapi-302326964Оценок пока нет
- Roscoe Vs HRMДокумент88 страницRoscoe Vs HRMCBC Nova ScotiaОценок пока нет
- Clinical SciencesДокумент6 страницClinical Sciencesapi-301251642Оценок пока нет
- Representation To The DGP and DigДокумент8 страницRepresentation To The DGP and DigAnil KumarОценок пока нет
- Parotidectomy: H.Shameer AhamedДокумент47 страницParotidectomy: H.Shameer AhamedAndreas RendraОценок пока нет