Вам также может понравиться
- Abortion: Mohamed Sinan Govt Medical College, CalicutДокумент60 страницAbortion: Mohamed Sinan Govt Medical College, CalicutYash SharmaОценок пока нет
- MiscarriageДокумент38 страницMiscarriagezianab aliОценок пока нет
- Abortion: Mohamed Sinan Govt Medical College, CalicutДокумент60 страницAbortion: Mohamed Sinan Govt Medical College, CalicutMhr AliОценок пока нет
- AbortionДокумент38 страницAbortiondimlyОценок пока нет
- 1 MiscarriageДокумент34 страницы1 Miscarriagezxcvbzaki123Оценок пока нет
- Abortion: TH THДокумент36 страницAbortion: TH THdimlyОценок пока нет
- Under Supervision Of: Dr. Enas AdnanДокумент9 страницUnder Supervision Of: Dr. Enas AdnanSarraa NajimОценок пока нет
- Ectopic Pregnancy - PowerpointДокумент60 страницEctopic Pregnancy - PowerpointAndrada Doţa100% (1)
- Obg AbortionДокумент62 страницыObg Abortionkashyap priyankaОценок пока нет
- Nursing Care of Clients With Reproductive Health ProblemsДокумент100 страницNursing Care of Clients With Reproductive Health ProblemsHassen ZabalaОценок пока нет
- Abortion: DEFINITION-Abortion Is The Separation Partial orДокумент77 страницAbortion: DEFINITION-Abortion Is The Separation Partial orPadmaОценок пока нет
- Care For The High Risk Pregnant ClientДокумент8 страницCare For The High Risk Pregnant ClientVanessa Marie ManzanoОценок пока нет
- Abortion Sept2021Документ51 страницаAbortion Sept2021vrunda joshiОценок пока нет
- Cervical InsufficiecyДокумент35 страницCervical InsufficiecyWilliams Emmanuel AdeyeyeОценок пока нет
- Circ LageДокумент54 страницыCirc Lagetsega tilahunОценок пока нет
- 14 Abortion Noted PDFДокумент37 страниц14 Abortion Noted PDFmohammed farajiОценок пока нет
- Prepared By: Aashma Bidari M.Sc. Nursing, 1 Year KusmsДокумент68 страницPrepared By: Aashma Bidari M.Sc. Nursing, 1 Year KusmsAasma BidariОценок пока нет
- AbortionДокумент62 страницыAbortionRaj KumarОценок пока нет
- Abortion ZeleДокумент49 страницAbortion ZeleZelalem DawitОценок пока нет
- Ectopic Pregnancy by EasterДокумент4 страницыEctopic Pregnancy by EasterIGA ABRAHAMОценок пока нет
- Induction of Labor-1Документ18 страницInduction of Labor-1Hariprasad V SОценок пока нет
- Recurrent Abortions: DR Seema Mehrotra Dept of Obstetrics and GynaecoloyДокумент85 страницRecurrent Abortions: DR Seema Mehrotra Dept of Obstetrics and GynaecoloyDrPraveen SharmaОценок пока нет
- First Trimester BleedingДокумент48 страницFirst Trimester BleedingEliana ArshidОценок пока нет
- AbortionДокумент42 страницыAbortionKondapavuluru Jyothi50% (2)
- Ob EmergenciesДокумент58 страницOb Emergenciessanthiyasandy100% (1)
- MK Disorders in Early Pregnancy (OBGY)Документ26 страницMK Disorders in Early Pregnancy (OBGY)Moses Jr KazevuОценок пока нет
- Abortion, Ectopic PregnancyДокумент139 страницAbortion, Ectopic PregnancyINFORMASI MENARIKОценок пока нет
- Female InfertilityДокумент33 страницыFemale InfertilityKiprotich Titus NgetichОценок пока нет
- Basic Infertility Work Up and Initial TreatmentДокумент46 страницBasic Infertility Work Up and Initial TreatmentHazel Fernandez VillarОценок пока нет
- In ComДокумент3 страницыIn ComDeen Deen L OrdonaОценок пока нет
- IUFDДокумент29 страницIUFDfasyanneshaОценок пока нет
- Ectopic Pregnancy RevisedДокумент44 страницыEctopic Pregnancy RevisedDegefaw BikoyОценок пока нет
- Book Picture Patient PictureДокумент22 страницыBook Picture Patient PictureAnsiya K AОценок пока нет
- Chorionic Villi SamplingДокумент4 страницыChorionic Villi SamplingSagar HanamasagarОценок пока нет
- Induction and Augmentation of LaborДокумент22 страницыInduction and Augmentation of LaborDagnachew kasaye100% (1)
- Cervical IncompetenceДокумент49 страницCervical Incompetencealadawi930Оценок пока нет
- Elizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyДокумент16 страницElizabeth G. Querubin BSN 3E1-9 - Group 195 A Ectopic PregnancyLizeth Querubin97% (38)
- 3&4 MiscarraigeДокумент90 страниц3&4 MiscarraigeAbdullah GadОценок пока нет
- Operatif DeliveryДокумент13 страницOperatif DeliveryPepo AryabarjaОценок пока нет
- Uterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseДокумент30 страницUterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseVijith.V.kumar80% (5)
- Obstetric HemorrhageДокумент74 страницыObstetric HemorrhageAmir KhanОценок пока нет
- EctopicДокумент42 страницыEctopicSafana NazeerОценок пока нет
- Gestational - PrematureДокумент3 страницыGestational - PrematureBench AvilaОценок пока нет
- Ectopic Pregnancy (Autosaved)Документ56 страницEctopic Pregnancy (Autosaved)susmita shresthaОценок пока нет
- Obsandgyne Tables 200pagesДокумент221 страницаObsandgyne Tables 200pagesRashed ShatnawiОценок пока нет
- Induction and Augmentation of LaborДокумент20 страницInduction and Augmentation of Laborjssamc prasootitantraОценок пока нет
- Obs. InvestigationsДокумент36 страницObs. InvestigationsSameena Rose AjmeriОценок пока нет
- Miscarriage Preterm Labor: Obstetrics and Gynecology Lyzikova Yu.AДокумент36 страницMiscarriage Preterm Labor: Obstetrics and Gynecology Lyzikova Yu.AMed PoxОценок пока нет
- 2-Complications of Pregnancy Pt1Документ37 страниц2-Complications of Pregnancy Pt1pavi7muruganathanОценок пока нет
- ObstetricemergenciesДокумент26 страницObstetricemergenciesrimshaafshenОценок пока нет
- Abortion and Ectopic PregnancyДокумент3 страницыAbortion and Ectopic PregnancyJefelson Eu Palaña NahidОценок пока нет
- Fetal Dev, AbortionДокумент128 страницFetal Dev, AbortionAr JayОценок пока нет
- AbortionДокумент32 страницыAbortionKirandeep ParmarОценок пока нет
- AbortionДокумент30 страницAbortionKIYAОценок пока нет
- Abortion: By: Priyanka Sadafule 1 Year PBBSC Student SeminarДокумент51 страницаAbortion: By: Priyanka Sadafule 1 Year PBBSC Student SeminarDigu SadafuleОценок пока нет
- Early Pregnancy Problems: Presented byДокумент28 страницEarly Pregnancy Problems: Presented byMalk OmryОценок пока нет
- Prenatal DiagnosisДокумент26 страницPrenatal DiagnosisShandy Suwanto PutraОценок пока нет
- Endometriosis: Li Qi LingДокумент67 страницEndometriosis: Li Qi LingwaheedaОценок пока нет
- In Endometriosis PCO Hyderosalpinx: BY Mahmoud Abd Ellatif Under Supervision of Prof. Mohamed HishamДокумент30 страницIn Endometriosis PCO Hyderosalpinx: BY Mahmoud Abd Ellatif Under Supervision of Prof. Mohamed HishamAhmed AnwarОценок пока нет
- Polycystic Ovarian SyndromeДокумент11 страницPolycystic Ovarian Syndromezianab aliОценок пока нет
- Contraception Part1Документ38 страницContraception Part1zianab aliОценок пока нет
- Gynaecological Laproscopy: By: DR - Hanaa Al-HeideryДокумент22 страницыGynaecological Laproscopy: By: DR - Hanaa Al-Heideryzianab aliОценок пока нет
- Operative ProcedureДокумент22 страницыOperative Procedurezianab aliОценок пока нет
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyДокумент11 страницContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliОценок пока нет
- Physiology of The Menstrual CycleДокумент17 страницPhysiology of The Menstrual Cyclezianab aliОценок пока нет
- Primary and Secondary Anenorrhea 2016-2017Документ24 страницыPrimary and Secondary Anenorrhea 2016-2017zianab ali100% (1)
- Female Genital Tract Anatomy 5th YearДокумент12 страницFemale Genital Tract Anatomy 5th Yearzianab aliОценок пока нет
- 1 CervixДокумент12 страниц1 Cervixzianab aliОценок пока нет
- FCM3-3.02 Philippine Cancer Control ProgramДокумент11 страницFCM3-3.02 Philippine Cancer Control ProgramJoher MendezОценок пока нет
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterДокумент4 страницыNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterJonas BagasОценок пока нет
- Symbicort LeafletДокумент10 страницSymbicort Leafletsheeno2607Оценок пока нет
- جورنال جاهزДокумент4 страницыجورنال جاهزasrd ramiОценок пока нет
- Speech & Language Therapy in Practice, Spring 1999Документ32 страницыSpeech & Language Therapy in Practice, Spring 1999Speech & Language Therapy in PracticeОценок пока нет
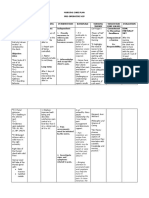
- Defining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions RationaleДокумент3 страницыDefining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions Rationalesbo100% (1)
- Community Medicine Notes & Question Bank: MBBS para ClinicalДокумент67 страницCommunity Medicine Notes & Question Bank: MBBS para ClinicalAnish Nazar100% (2)
- Bartholin CystДокумент6 страницBartholin CystCokorda Istri Devi LarayanthiОценок пока нет
- Arthritis PDFДокумент3 страницыArthritis PDFMiguel Cuevas DolotОценок пока нет
- F 360Документ6 страницF 360اسعد عبد الحميد50% (2)
- JA3 Adam Ong DoctorДокумент7 страницJA3 Adam Ong DoctorakosiemОценок пока нет
- Breast Cancer PathophysiologyДокумент17 страницBreast Cancer PathophysiologySwit Tapican MaangОценок пока нет
- Protein Energy Malnutrition - 2Документ32 страницыProtein Energy Malnutrition - 2J V SamuelОценок пока нет
- Abnormal PuerperiumДокумент21 страницаAbnormal PuerperiumNatukunda DianahОценок пока нет
- Degenerative Disc Disease (Spondylosis)Документ4 страницыDegenerative Disc Disease (Spondylosis)klockОценок пока нет
- Best Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihДокумент7 страницBest Guest Lecturer of Ars University Materi Gizi Asam Urat Nila Sukma RatihARS University BandungОценок пока нет
- Transfusion in TraumaДокумент28 страницTransfusion in TraumaSyeda Nasra ShahОценок пока нет
- Arthritis Case Presentation - Dr. KlaesДокумент27 страницArthritis Case Presentation - Dr. KlaesShanti VennamОценок пока нет
- Alcohol Abuse and DependenceДокумент10 страницAlcohol Abuse and Dependencezig6yОценок пока нет
- Ren 15Документ2 страницыRen 15ray72roОценок пока нет
- Antiemesis NCCNДокумент79 страницAntiemesis NCCNana salazarОценок пока нет
- 7.1. Anemia 2023Документ30 страниц7.1. Anemia 2023MichellyTjoaОценок пока нет
- Pillitteri: Maternal and Child Health Nursing, 5 EditionДокумент9 страницPillitteri: Maternal and Child Health Nursing, 5 EditionJoy CalimlimОценок пока нет
- Nursing Care PlanДокумент30 страницNursing Care PlanJam CorrosОценок пока нет
- Pregnancy Induced Hypertension PathophysiologyДокумент2 страницыPregnancy Induced Hypertension PathophysiologyCamille Grace100% (1)
- DR - Nerve Second Year QBДокумент123 страницыDR - Nerve Second Year QBvillagemasalahutОценок пока нет
- Esophageal Atresia: Elvita Rahmi DaulayДокумент21 страницаEsophageal Atresia: Elvita Rahmi DaulayabdullahshiddiqadamОценок пока нет
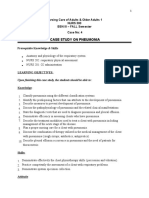
- The Case of Mr. Mohammad With Pneumonia Pleural EffusionДокумент6 страницThe Case of Mr. Mohammad With Pneumonia Pleural EffusionjanaОценок пока нет
- Neural Tube DefectsДокумент4 страницыNeural Tube DefectsReyniel Pablo ElumbaОценок пока нет
- UKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022Документ1 страницаUKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022cicitОценок пока нет
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeОт EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeРейтинг: 3.5 из 5 звезд3.5/5 (13)
- Skinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!От EverandSkinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!Рейтинг: 3.5 из 5 звезд3.5/5 (489)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeОт EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeОценок пока нет
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayОт EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayРейтинг: 4.5 из 5 звезд4.5/5 (3)
- What to Expect When You’re Expecting (5th Edition)От EverandWhat to Expect When You’re Expecting (5th Edition)Рейтинг: 5 из 5 звезд5/5 (1)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenОт EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenРейтинг: 4 из 5 звезд4/5 (154)
- First Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!От EverandFirst Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!Рейтинг: 5 из 5 звезд5/5 (21)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouОт EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouОценок пока нет
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisОт EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisРейтинг: 3 из 5 звезд3/5 (2)
- The Strength and Conditioning Bible: How to Train Like an AthleteОт EverandThe Strength and Conditioning Bible: How to Train Like an AthleteОценок пока нет
- Reclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeОт EverandReclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeРейтинг: 5 из 5 звезд5/5 (16)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!От EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Рейтинг: 5 из 5 звезд5/5 (1)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondОт EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondРейтинг: 4.5 из 5 звезд4.5/5 (3)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.От EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Рейтинг: 4.5 из 5 звезд4.5/5 (128)
- Get the Guy On Your Terms: Proven Dating Advice for Women to Attract Men, Find Love and Build a Relationship that LastsОт EverandGet the Guy On Your Terms: Proven Dating Advice for Women to Attract Men, Find Love and Build a Relationship that LastsРейтинг: 5 из 5 звезд5/5 (18)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersОт EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersРейтинг: 4.5 из 5 звезд4.5/5 (72)
- Women's Brains: The Female Brain Explained through Neural AnalysesОт EverandWomen's Brains: The Female Brain Explained through Neural AnalysesРейтинг: 4.5 из 5 звезд4.5/5 (22)
- WomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceОт EverandWomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceРейтинг: 4.5 из 5 звезд4.5/5 (91)
- Awakening Fertility: The Essential Art of Preparing for PregnancyОт EverandAwakening Fertility: The Essential Art of Preparing for PregnancyРейтинг: 4.5 из 5 звезд4.5/5 (36)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysОт EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysРейтинг: 4.5 из 5 звезд4.5/5 (5)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeОт EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeРейтинг: 4 из 5 звезд4/5 (15)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityОт EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityРейтинг: 4.5 из 5 звезд4.5/5 (12)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.От EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Рейтинг: 3.5 из 5 звезд3.5/5 (7)
- Nurture: A Modern Guide to Pregnancy, Birth, Early Motherhood—and Trusting Yourself and Your BodyОт EverandNurture: A Modern Guide to Pregnancy, Birth, Early Motherhood—and Trusting Yourself and Your BodyРейтинг: 4.5 из 5 звезд4.5/5 (14)
- Intoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingОт EverandIntoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingРейтинг: 5 из 5 звезд5/5 (1)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouОт EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouРейтинг: 4 из 5 звезд4/5 (25)