Вам также может понравиться
- Park PlaceДокумент41 страницаPark PlaceNBC MontanaОценок пока нет
- Brooke Knoll Village ReportДокумент14 страницBrooke Knoll Village ReportFOX59/CBS4Оценок пока нет
- Crest 2020Документ12 страницCrest 2020NBC MontanaОценок пока нет
- Crest Health 2020 JanuaryДокумент57 страницCrest Health 2020 JanuaryNBC MontanaОценок пока нет
- 321Z47Q 0qte9xcys007sx5 PDFДокумент6 страниц321Z47Q 0qte9xcys007sx5 PDFNBC MontanaОценок пока нет
- PRINTED: 01/03/2022 Form Approved: (X5) Completion DateДокумент19 страницPRINTED: 01/03/2022 Form Approved: (X5) Completion DateNBC MontanaОценок пока нет
- University Place Maggots ComplaintДокумент17 страницUniversity Place Maggots ComplaintJoseph GillОценок пока нет
- Marshwood 3-17-20 Statement of DeficienciesДокумент17 страницMarshwood 3-17-20 Statement of DeficienciesMaine Trust For Local NewsОценок пока нет
- Report On Silver Oak Nursing and Rehabilitation CenterДокумент112 страницReport On Silver Oak Nursing and Rehabilitation CenterA.W. CarrosОценок пока нет
- Statement of Deficiencies and Plan of Correction 8/10/2020Документ32 страницыStatement of Deficiencies and Plan of Correction 8/10/2020Maine Trust For Local NewsОценок пока нет
- Iroquois Nursing Home Inspection ReportДокумент25 страницIroquois Nursing Home Inspection ReportJames Mulder100% (1)
- ODH Report On MontefioreДокумент63 страницыODH Report On MontefioreWKYC.com100% (1)
- Whitefish Care 2020 Inspection DrugsДокумент18 страницWhitefish Care 2020 Inspection DrugsNBC MontanaОценок пока нет
- Van Duyn June 21, 2021 InspectionДокумент106 страницVan Duyn June 21, 2021 InspectionJames Mulder100% (1)
- 321Z3D2 0KD8D6L7P001F6G PDFДокумент13 страниц321Z3D2 0KD8D6L7P001F6G PDFNBC MontanaОценок пока нет
- Whitefish CareДокумент32 страницыWhitefish CareNBC MontanaОценок пока нет
- Van Duyn May 11, 2021 InspectionДокумент12 страницVan Duyn May 11, 2021 InspectionJames MulderОценок пока нет
- Stearns COVID-19 Inspection ReportДокумент54 страницыStearns COVID-19 Inspection ReportLexi CortesОценок пока нет
- Torrance State Hospital Inspection ReportДокумент5 страницTorrance State Hospital Inspection ReportEd MahonОценок пока нет
- Whitefish C and R Sept 2020Документ18 страницWhitefish C and R Sept 2020NBC MontanaОценок пока нет
- Department of Health and Human Services Inspection ReportДокумент51 страницаDepartment of Health and Human Services Inspection ReportWCNC DigitalОценок пока нет
- Onondaga Center Inspection ReportДокумент33 страницыOnondaga Center Inspection ReportJames MulderОценок пока нет
- Jewish Home of CNY Inspection ReportДокумент60 страницJewish Home of CNY Inspection ReportJames MulderОценок пока нет
- Bishop Rehabilitation Inspection ReportДокумент18 страницBishop Rehabilitation Inspection ReportJames MulderОценок пока нет
- Van Rensselaer Manor Statement of DeficiencyДокумент5 страницVan Rensselaer Manor Statement of DeficiencyBethanyОценок пока нет
- Continental CareДокумент58 страницContinental CareNBC MontanaОценок пока нет
- Bishop Rehabilitation and Nursing Center Inspection ReportДокумент117 страницBishop Rehabilitation and Nursing Center Inspection ReportJames MulderОценок пока нет
- ReportДокумент73 страницыReportDean Welte - KTIVОценок пока нет
- Statement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)Документ12 страницStatement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)NTV NewsОценок пока нет
- Central Maine Medical Center Letters and SurveysДокумент39 страницCentral Maine Medical Center Letters and SurveysMaine Trust For Local News100% (1)
- State Fire Marshal's Report On Carilion Roanoke Memorial Hospital's Fire Safety ViolationsДокумент352 страницыState Fire Marshal's Report On Carilion Roanoke Memorial Hospital's Fire Safety ViolationsrtimesОценок пока нет
- James Square ViolationsДокумент66 страницJames Square ViolationsNewsChannel 9Оценок пока нет
- MD Anderson A-2567Документ268 страницMD Anderson A-2567Houston Chronicle50% (2)
- Arbor Court DIA ReportДокумент6 страницArbor Court DIA ReportLocal 5 News (WOI-TV)Оценок пока нет
- Dept. of Health Wellspan Death ReportДокумент44 страницыDept. of Health Wellspan Death ReportAnonymous nhLKKmcDОценок пока нет
- Missoula Care RehabДокумент37 страницMissoula Care RehabNBC MontanaОценок пока нет
- UPMC Memorial Bedford Hospital ViolationsДокумент119 страницUPMC Memorial Bedford Hospital ViolationsJacquelyn GrayОценок пока нет
- Faith GardensДокумент42 страницыFaith GardensJacquelyn GrayОценок пока нет
- LGH InspectionДокумент22 страницыLGH InspectionTravis KellarОценок пока нет
- Oregon State Junction City 90 Day Term SOD 05052022Документ134 страницыOregon State Junction City 90 Day Term SOD 05052022Sinclair Broadcast Group - EugeneОценок пока нет
- OCDC 2023 Health InspectionДокумент9 страницOCDC 2023 Health InspectionDavid MarkОценок пока нет
- Oklahoma Department of Health On Conditions at Oklahoma County JailДокумент39 страницOklahoma Department of Health On Conditions at Oklahoma County JailAnonymous EHPq5k100% (1)
- Heights of Summerlin Statement of DeficienciesДокумент26 страницHeights of Summerlin Statement of DeficienciesLas Vegas Review-JournalОценок пока нет
- Inspection Report 3 Texoma Medical Center and TMC Behavioral Health CenterДокумент18 страницInspection Report 3 Texoma Medical Center and TMC Behavioral Health CentermilesmoffeitОценок пока нет
- Bel Pre MD - Feb 2022 InvestigationДокумент15 страницBel Pre MD - Feb 2022 InvestigationMichael Scott DavidsonОценок пока нет
- Survey Report For 450388 - 4.29.2019Документ14 страницSurvey Report For 450388 - 4.29.2019Express-NewsОценок пока нет
- Complaint 2Документ7 страницComplaint 2gtqtmd6xszОценок пока нет
- Newark Care and Rehab COVID-19 ReportДокумент39 страницNewark Care and Rehab COVID-19 ReportblankamncoОценок пока нет
- Original CDPH SurveyДокумент53 страницыOriginal CDPH SurveyJames WardОценок пока нет
- New Hanover Treatment Center - 2017 DHHS Inspection (Redacted)Документ50 страницNew Hanover Treatment Center - 2017 DHHS Inspection (Redacted)Ben SchachtmanОценок пока нет
- Parkview Healthcare Inspection ReportДокумент84 страницыParkview Healthcare Inspection ReportGreg DaileyОценок пока нет
- Black Hills Children's Home Deficiencies - DennardДокумент2 страницыBlack Hills Children's Home Deficiencies - DennardJacquelyn GrayОценок пока нет
- Latest Medicare Health Inspections For Nursing Homes Owned by Bob DeanДокумент70 страницLatest Medicare Health Inspections For Nursing Homes Owned by Bob DeanWWLTVWebteamОценок пока нет
- Abortion Clinic Deficiency ReportДокумент3 страницыAbortion Clinic Deficiency ReportMike CasonОценок пока нет
- Desert Valley Hospital - SepticemiaДокумент3 страницыDesert Valley Hospital - SepticemiaefjbarreraОценок пока нет
- Construction Liens for the Pacific Northwest Alaska Idaho Oregon Washington Federal Public Works: A PrimerОт EverandConstruction Liens for the Pacific Northwest Alaska Idaho Oregon Washington Federal Public Works: A PrimerОценок пока нет
- Guidelines for Safe Automation of Chemical ProcessesОт EverandGuidelines for Safe Automation of Chemical ProcessesОценок пока нет
- Delivering Water and Power: GIS for UtilitiesОт EverandDelivering Water and Power: GIS for UtilitiesPat HohlРейтинг: 4 из 5 звезд4/5 (1)
- Precis - Reaching Teaching TraumaДокумент3 страницыPrecis - Reaching Teaching TraumaRay StillОценок пока нет
- Face Mask Pattern: MenДокумент1 страницаFace Mask Pattern: MenRay StillОценок пока нет
- June 10, 2020 - The Courier-HeraldДокумент16 страницJune 10, 2020 - The Courier-HeraldRay Still0% (1)
- Enumclaw/St. Elizabeth Vaccine FlyerДокумент1 страницаEnumclaw/St. Elizabeth Vaccine FlyerRay StillОценок пока нет
- Allen Bittner ComplaintДокумент3 страницыAllen Bittner ComplaintRay StillОценок пока нет
- Enumclaw High School Leadership Letter To School AdministrationДокумент1 страницаEnumclaw High School Leadership Letter To School AdministrationRay Still100% (1)
- JoHanna Pratt Estate v. Rainier School - Defendants AnswerДокумент10 страницJoHanna Pratt Estate v. Rainier School - Defendants AnswerRay StillОценок пока нет
- Precis-The Connected ChildДокумент3 страницыPrecis-The Connected ChildRay StillОценок пока нет
- Black Diamond Council Fire Study Presentation - PUBLISHED 12.18.2020Документ26 страницBlack Diamond Council Fire Study Presentation - PUBLISHED 12.18.2020Ray StillОценок пока нет
- King County Motion To Intervene in Waste Action Project v. Buckley Recycle CenterДокумент22 страницыKing County Motion To Intervene in Waste Action Project v. Buckley Recycle CenterRay StillОценок пока нет
- Enumclaw Pumpkin Contest RegistrationДокумент1 страницаEnumclaw Pumpkin Contest RegistrationRay StillОценок пока нет
- Notice of Termination and Intent To RenegotiateДокумент3 страницыNotice of Termination and Intent To RenegotiateRay StillОценок пока нет
- Estate of JoHanna Pratt v. Rainier SchoolДокумент8 страницEstate of JoHanna Pratt v. Rainier SchoolRay StillОценок пока нет
- Thomas Superseding IndictmentДокумент14 страницThomas Superseding IndictmentRay StillОценок пока нет
- GOP Lawsuit Against Gov. Jay Inslee's Emergency Lockdown in WAДокумент28 страницGOP Lawsuit Against Gov. Jay Inslee's Emergency Lockdown in WARay StillОценок пока нет
- Hand Sewn Face Mask Instructions From CHI FranciscanДокумент7 страницHand Sewn Face Mask Instructions From CHI FranciscanRay StillОценок пока нет
- Koler, Glenn, and Bremner Complaint Against Black DiamondДокумент18 страницKoler, Glenn, and Bremner Complaint Against Black DiamondRay StillОценок пока нет
- Allan and Joann Thomas ComplaintДокумент23 страницыAllan and Joann Thomas ComplaintRay StillОценок пока нет
- Black Diamond Response To Koler, Glenn, and Bremner ComplaintДокумент13 страницBlack Diamond Response To Koler, Glenn, and Bremner ComplaintRay StillОценок пока нет
- Washington State Auditor's Office Report On King County Drainage District 5Документ7 страницWashington State Auditor's Office Report On King County Drainage District 5Ray StillОценок пока нет
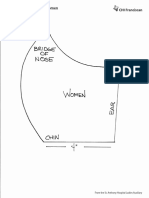
- Face Mask Pattern: WomenДокумент1 страницаFace Mask Pattern: WomenRay StillОценок пока нет
- Enumclaw City Council Public Safety Committee Library Survey ResultsДокумент74 страницыEnumclaw City Council Public Safety Committee Library Survey ResultsRay StillОценок пока нет
- Additional Reagan Dunn/Allan Thomas CorrespondenceДокумент1 страницаAdditional Reagan Dunn/Allan Thomas CorrespondenceRay StillОценок пока нет
- Reagan Dunn/Allan Thomas CorrespondenceДокумент10 страницReagan Dunn/Allan Thomas CorrespondenceRay StillОценок пока нет
- 2018 Annual Summary Homeless Deaths - King CountyДокумент3 страницы2018 Annual Summary Homeless Deaths - King CountyRay StillОценок пока нет
- All Is Fair: Weigh in On Driving SR 410Документ20 страницAll Is Fair: Weigh in On Driving SR 410Ray StillОценок пока нет
- 2 Hurt in Ultralight Crash: We Don't Want To See It Fall Away'Документ20 страниц2 Hurt in Ultralight Crash: We Don't Want To See It Fall Away'Ray StillОценок пока нет
- Wisconsin HOPE Lab Still Hungry and HomelessДокумент52 страницыWisconsin HOPE Lab Still Hungry and Homelesstele6Оценок пока нет
- Ech 102418Документ28 страницEch 102418Ray StillОценок пока нет
- Nutritional assessment pregnancy lactationДокумент11 страницNutritional assessment pregnancy lactationKathleen Martinez100% (1)
- Osteomyelitis HandoutДокумент4 страницыOsteomyelitis HandoutJazzmin Angel ComalingОценок пока нет
- Zinc Oxide-Eugenol and Calcium HydroxideДокумент5 страницZinc Oxide-Eugenol and Calcium HydroxideJulioОценок пока нет
- Electo Homeopathy MedicinesДокумент3 страницыElecto Homeopathy MedicinesKoushik MaitraОценок пока нет
- Hubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasiДокумент17 страницHubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasidrelvОценок пока нет
- OB Case Presentation Inforgraphic Garcia-GumbeДокумент2 страницыOB Case Presentation Inforgraphic Garcia-GumbeLara GeeОценок пока нет
- Organ Systems ComparisonДокумент12 страницOrgan Systems ComparisonJeffrey YumangОценок пока нет
- Halozyme Therapeutics, Inc. 2009 Investor Day PresentationДокумент88 страницHalozyme Therapeutics, Inc. 2009 Investor Day Presentationsstrumello7395Оценок пока нет
- BDSДокумент3 страницыBDScristalmae16Оценок пока нет
- E NihssДокумент5 страницE NihssNayeli SánchezОценок пока нет
- Drug Study Quinine SulfateДокумент7 страницDrug Study Quinine SulfateKathlyn_Matic_6376Оценок пока нет
- NDT 3 429Документ13 страницNDT 3 429Mohammed AldaffaieОценок пока нет
- Microbiology Quick TableДокумент2 страницыMicrobiology Quick TableCoy Nuñez100% (2)
- Practical Research 2Документ66 страницPractical Research 2Cris Antonette AbataОценок пока нет
- MODUL 1 FKG UnairДокумент61 страницаMODUL 1 FKG UnairLaurensia NovenОценок пока нет
- Review 02Документ2 страницыReview 02Vicki KimОценок пока нет
- Capalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosДокумент10 страницCapalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosJorge Alberto Salazar CartinОценок пока нет
- Prosthetic Management - Transtibial Amputation Part 12Документ25 страницProsthetic Management - Transtibial Amputation Part 12Marizandi BothaОценок пока нет
- ABO Blood Group SystemДокумент61 страницаABO Blood Group Systemmail2jackal50% (2)
- SOP 6-Minute-Walk Test 1. General Considerations: 6-Minute Walking Distance: Covered Distance inДокумент5 страницSOP 6-Minute-Walk Test 1. General Considerations: 6-Minute Walking Distance: Covered Distance inadeОценок пока нет
- A5 Pig Management GuidlinesДокумент4 страницыA5 Pig Management GuidlinesAnna NdunaОценок пока нет
- Talk WslidesДокумент43 страницыTalk WslidesraydonalОценок пока нет
- Nephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassДокумент143 страницыNephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassKay BristolОценок пока нет
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFДокумент1 страницаSteroid Tapering and Supportive Treatment Guidance V1.0 PDFNthutagaol TrusОценок пока нет
- Barrier Free ArchitectureДокумент3 страницыBarrier Free ArchitectureAmarjit SahОценок пока нет
- NCMB316 Rle 2-10-7addison's DiseaseДокумент4 страницыNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaОценок пока нет
- HYPETHYROIDISM NURSING CARE PLANДокумент6 страницHYPETHYROIDISM NURSING CARE PLANTrisha Joyce MadriagaОценок пока нет
- Developing Biocompatibility For Medical DevicesДокумент30 страницDeveloping Biocompatibility For Medical DevicesNagula Naresh100% (1)
- CANINE-Pathophysiology of Organ Failure in Severe Acute Pancreatitis in DogsДокумент10 страницCANINE-Pathophysiology of Organ Failure in Severe Acute Pancreatitis in Dogstaner_soysurenОценок пока нет
- Text Book of Sarcoidosis With Homeopathy TreatmentДокумент107 страницText Book of Sarcoidosis With Homeopathy TreatmentDr. Rajneesh Kumar Sharma MD Hom100% (4)