Вам также может понравиться
- Datasheet Wonderware InTouch EN PDFДокумент16 страницDatasheet Wonderware InTouch EN PDFGuillermo Osvaldo Rivera MelladoОценок пока нет
- WhitePaper Cloud Based SCADA SystemsДокумент12 страницWhitePaper Cloud Based SCADA SystemsSuman Kumar SinghОценок пока нет
- Cloud Computing 101Документ24 страницыCloud Computing 101Suman Kumar SinghОценок пока нет
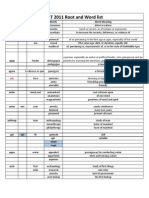
- List of RootsДокумент15 страницList of RootsRaja NagaiahОценок пока нет
- Forex Signal SitesДокумент3 страницыForex Signal SitesSuman Kumar SinghОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- BPT GTT & Diabetes MellitusДокумент25 страницBPT GTT & Diabetes MellitusBalajiОценок пока нет
- The Endocrine Glands & Their HormonesДокумент35 страницThe Endocrine Glands & Their HormonesEtta Sagita Leonora100% (1)
- Quiz 1 2017 AnswersДокумент35 страницQuiz 1 2017 Answershercules 007Оценок пока нет
- Fornas 011113Документ71 страницаFornas 011113Endah susantiОценок пока нет
- Gestational Diabetes Case StudyДокумент28 страницGestational Diabetes Case StudyCruz, Donna Angela M.Оценок пока нет
- E Katalog BaruДокумент31 страницаE Katalog BaruAnna ApriyantiОценок пока нет
- Diabetes EssayДокумент7 страницDiabetes Essayapi-315440977Оценок пока нет
- I3 ProposalДокумент11 страницI3 Proposalrajeev_995445030Оценок пока нет
- Green TeaДокумент12 страницGreen TeaSaraah GhoriОценок пока нет
- Fasting 3 - Jason - FungДокумент16 страницFasting 3 - Jason - FungNyala100% (2)
- DIABETESДокумент44 страницыDIABETESJessa MaeОценок пока нет
- Literature Review 2Документ4 страницыLiterature Review 2api-582849036Оценок пока нет
- Diabetes MellitusДокумент18 страницDiabetes Mellitusrajirajesh100% (1)
- Guidance for Industry on Developing Drugs for Diabetes TreatmentДокумент34 страницыGuidance for Industry on Developing Drugs for Diabetes Treatmentbmartindoyle6396Оценок пока нет
- Endocrine HarmonyДокумент68 страницEndocrine HarmonyafnanОценок пока нет
- Pink Panther - Diabetes Management - Chapter 1Документ6 страницPink Panther - Diabetes Management - Chapter 1jennmoyerОценок пока нет
- Insulin Plant. Science NewsДокумент2 страницыInsulin Plant. Science NewsJames TabioloОценок пока нет
- Anatomy and PhysiologyДокумент2 страницыAnatomy and PhysiologyJeffrey Calicdan BucalaОценок пока нет
- Diabetes WikiДокумент30 страницDiabetes WikiUnggul YudhaОценок пока нет
- Natural Muscle - April 2008Документ33 страницыNatural Muscle - April 2008alfortlan100% (1)
- Handy Health Guide To DiabetesДокумент49 страницHandy Health Guide To DiabetesDiabetes Care100% (1)
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaДокумент5 страницDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいОценок пока нет
- Hypoglycemia Protocol for Diabetics and Non-DiabeticsДокумент43 страницыHypoglycemia Protocol for Diabetics and Non-DiabeticsHEBA NAJJAR100% (1)
- Managing Diabetes with Diet and ExerciseДокумент32 страницыManaging Diabetes with Diet and ExerciseNor Hikmah HarisОценок пока нет
- The Prime Cause of Type-2 (T2D), Type-1 Diabetes (T1D) and The Relation Between Diabetes and CancerДокумент11 страницThe Prime Cause of Type-2 (T2D), Type-1 Diabetes (T1D) and The Relation Between Diabetes and CancerSorushОценок пока нет
- Fasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheДокумент4 страницыFasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheYOG.GANAR2291Оценок пока нет
- Insulin Resistance by DR Sidra SadiqДокумент34 страницыInsulin Resistance by DR Sidra Sadiqdr. SheryarOrakzaiОценок пока нет
- Sam Dagogo-Jack Eds. Diabetes Mellitus in Developing Countries and Underserved CommunitiesДокумент299 страницSam Dagogo-Jack Eds. Diabetes Mellitus in Developing Countries and Underserved CommunitiesTuan NguyenОценок пока нет
- Oral Antidiabetic Drugs 2017BДокумент39 страницOral Antidiabetic Drugs 2017BDineish MurugaiahОценок пока нет
- The History of Diabetes MellitusДокумент3 страницыThe History of Diabetes Mellitusjoummana mОценок пока нет