Вам также может понравиться
- The Quality of Life ScaleДокумент15 страницThe Quality of Life ScaleMohamed Elsayed0% (1)
- Quality Life Scale PDFДокумент7 страницQuality Life Scale PDFFayza RihastaraОценок пока нет
- 1 s2.0 S1561541309600442 Main PDFДокумент6 страниц1 s2.0 S1561541309600442 Main PDFDinas Perpustakaan Daerah DispusdaОценок пока нет
- Findings From Britain: The Effects Illness Quality of Households in GreatДокумент7 страницFindings From Britain: The Effects Illness Quality of Households in GreatGunung MahameruОценок пока нет
- Saúde e Bem-Estar de Lésbicas, Gays, Bissexuais, Transgêneros e Intersexuais Com 50 Anos Ou MaisДокумент6 страницSaúde e Bem-Estar de Lésbicas, Gays, Bissexuais, Transgêneros e Intersexuais Com 50 Anos Ou MaisRodrigo AristidesОценок пока нет
- BJC 2015310 AДокумент12 страницBJC 2015310 AJuliana SoaresОценок пока нет
- The Chinese Version of The World Health Organization Quality of Life Instrument-Older Adults Module (WHOQOL-OLD) : Psychometric EvaluationДокумент8 страницThe Chinese Version of The World Health Organization Quality of Life Instrument-Older Adults Module (WHOQOL-OLD) : Psychometric EvaluationSyed ShahОценок пока нет
- Measures To Protect Health Workers From Exposure To Infectious DiseasesДокумент20 страницMeasures To Protect Health Workers From Exposure To Infectious Diseasesk ucheОценок пока нет
- The Norwegian Version of The Quality of Life Scale (QOLS-N)Документ8 страницThe Norwegian Version of The Quality of Life Scale (QOLS-N)Andreea OniceanuОценок пока нет
- Quality of Life Enjoyment and Satisfaction QuestionnaireДокумент8 страницQuality of Life Enjoyment and Satisfaction QuestionnairekarinadapariaОценок пока нет
- Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related?Документ11 страницAgeism, Healthy Life Expectancy and Population Ageing: How Are They Related?Betsabé CastroОценок пока нет
- Quality of Life in Patients With End Stage Renal Disease On HemodialysisДокумент11 страницQuality of Life in Patients With End Stage Renal Disease On HemodialysisAmalia UtamiОценок пока нет
- Body Mass IndexДокумент6 страницBody Mass Indexayu yuliantiОценок пока нет
- To What Extent Do Oral Disorders Compromise The Quality of LifeДокумент10 страницTo What Extent Do Oral Disorders Compromise The Quality of LifeAhmad Ulil AlbabОценок пока нет
- Article MSQOL-54Документ21 страницаArticle MSQOL-54bogdanneamtuОценок пока нет
- Qlis - Development of A Schizophrenia-Specific Quality-Of-Life ScaleДокумент12 страницQlis - Development of A Schizophrenia-Specific Quality-Of-Life ScaleAnonymous hvOuCjОценок пока нет
- Quality of Life of Filipino Cancer PatientsДокумент2 страницыQuality of Life of Filipino Cancer PatientsApril Garcia MayoОценок пока нет
- Assessment of Quality of Life Among Children With End-Stage Renal Disease: A Cross-Sectional StudyДокумент7 страницAssessment of Quality of Life Among Children With End-Stage Renal Disease: A Cross-Sectional StudysavitageraОценок пока нет
- Quality of Life in Epilepsy: A Study of Brazilian AdolescentsДокумент9 страницQuality of Life in Epilepsy: A Study of Brazilian Adolescentsnathália_siqueira_47Оценок пока нет
- Quality of Life in Patients With Neurogenic DysphagiaДокумент8 страницQuality of Life in Patients With Neurogenic DysphagiaDaniela OrtizОценок пока нет
- Qol in DialysisДокумент6 страницQol in Dialysism29hereОценок пока нет
- Brazilian Version of A Lifestyle QuestionnaireДокумент7 страницBrazilian Version of A Lifestyle QuestionnaireAntônio de LimaОценок пока нет
- EATING DISORDERS Research ProposalДокумент12 страницEATING DISORDERS Research ProposalKhushi KashyapОценок пока нет
- PIIS1059131118301237Документ8 страницPIIS1059131118301237bilal hadiОценок пока нет
- Development of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Документ12 страницDevelopment of A Health-Related Quality-of-Life Questionnaire (PCOSQ) For Women With Polycystic Ovary Syndrome (PCOS)Ke XuОценок пока нет
- Ecohis OriginalДокумент10 страницEcohis OriginalShahid ShaikhОценок пока нет
- QualidadeVida Crianças DoençacronicaДокумент9 страницQualidadeVida Crianças DoençacronicaCláudia OliveiraОценок пока нет
- Roundtable On Quality of Life (QOL) : Menopause ManagementДокумент4 страницыRoundtable On Quality of Life (QOL) : Menopause ManagementTommy FebriantoОценок пока нет
- Research ArticleДокумент8 страницResearch Articlewoldekidansamuel299Оценок пока нет
- 09 - Active Life Expectancy of Filipino Older PeopleДокумент16 страниц09 - Active Life Expectancy of Filipino Older PeopleAfanie Mae Romero EstepaОценок пока нет
- Aging, Gender and Quality of Life (AGEQOL) Study: Factors Associated With Good Quality of Life in Older Brazilian Community-Dwelling AdultsДокумент11 страницAging, Gender and Quality of Life (AGEQOL) Study: Factors Associated With Good Quality of Life in Older Brazilian Community-Dwelling AdultsNanaОценок пока нет
- Paper Impact of Overweight and Obesity On Health-Related Quality of Life - A Swedish Population StudyДокумент8 страницPaper Impact of Overweight and Obesity On Health-Related Quality of Life - A Swedish Population Studyuswatun khasanahОценок пока нет
- 1887 117407-Numans 2014, Validity and Reliability of The KatzДокумент7 страниц1887 117407-Numans 2014, Validity and Reliability of The KatzAhmed DiabОценок пока нет
- P122Документ10 страницP122Vicho Neira PinochetОценок пока нет
- Wellness BehaviourДокумент2 страницыWellness BehaviourJohn Paul Ta PhamОценок пока нет
- Lifestyle of The Elderly Living in Rural and Urban Areas Measured by The FANTASTIC Life InventoryДокумент6 страницLifestyle of The Elderly Living in Rural and Urban Areas Measured by The FANTASTIC Life InventoryLuana FerreiraОценок пока нет
- Original PapersДокумент8 страницOriginal Papersرقية ياسينОценок пока нет
- Sedentary + SuicideДокумент22 страницыSedentary + SuicideScribdMeUpОценок пока нет
- Disability, Frailty and Depression in The Community-Dwelling Older Adults With OsteosarcopeniaДокумент7 страницDisability, Frailty and Depression in The Community-Dwelling Older Adults With OsteosarcopeniaKhairunnisa Ayu KresnandaОценок пока нет
- Quality of Life in Glaucoma: A Review of The LiteratureДокумент23 страницыQuality of Life in Glaucoma: A Review of The LiteratureMakhda Nurfatmala LОценок пока нет
- 2010 Dorn - ColiacДокумент10 страниц2010 Dorn - Coliacnermal93Оценок пока нет
- Public HealthДокумент9 страницPublic HealthMarília LuzОценок пока нет
- 2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceДокумент9 страниц2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceMarietta_MonariОценок пока нет
- Journal of A Ffective Disorders: Research PaperДокумент7 страницJournal of A Ffective Disorders: Research PaperangelavillateavilaОценок пока нет
- 2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionДокумент16 страниц2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionEsteysi Villarroel BernalesОценок пока нет
- Health Literacy and Ethnic Disparities in Health-Related Quality of Life Among Rural Women: Results From A Chinese Poor Minority AreaДокумент9 страницHealth Literacy and Ethnic Disparities in Health-Related Quality of Life Among Rural Women: Results From A Chinese Poor Minority AreaAndriani SittiОценок пока нет
- QoL Obese ChildrenДокумент7 страницQoL Obese ChildrenLiga Sabatina de BaloncestoОценок пока нет
- FANTASTIC Lifestyle AssessmentДокумент6 страницFANTASTIC Lifestyle AssessmentzacОценок пока нет
- Health and Quality of Life OutcomesДокумент7 страницHealth and Quality of Life OutcomesvinayakОценок пока нет
- Rhinosinusitis - Its Impact On Quality of Life: 3 Medical Faculty of Charles University, Prague Czech RepublicДокумент25 страницRhinosinusitis - Its Impact On Quality of Life: 3 Medical Faculty of Charles University, Prague Czech RepublicBlebea CristinaОценок пока нет
- 1 PBДокумент6 страниц1 PBMiranda Yudhi CyubidubiduuОценок пока нет
- The First Article We Will Review and Critique Where Relevant Is 'Документ4 страницыThe First Article We Will Review and Critique Where Relevant Is 'Onkwani DavidОценок пока нет
- En V50n4a06 PDFДокумент8 страницEn V50n4a06 PDFmeriza dahliaОценок пока нет
- (PCOSQ) ImpДокумент12 страниц(PCOSQ) Impamanysalama5976Оценок пока нет
- EДокумент375 страницEANA MARIA CRISTIANAОценок пока нет
- Saracli Et Al 2015Документ7 страницSaracli Et Al 2015Henry WijayaОценок пока нет
- QV STUDY 2012 Quality of Life of Methilfenidate Treatment - Pin-ChenДокумент6 страницQV STUDY 2012 Quality of Life of Methilfenidate Treatment - Pin-ChenDoniLeiteОценок пока нет
- 3612-Article Text-12854-2-10-20240108Документ12 страниц3612-Article Text-12854-2-10-202401084ymwg78wxcОценок пока нет
- Quality of Life in Patients With Chronic PDFДокумент12 страницQuality of Life in Patients With Chronic PDFInsane BryОценок пока нет
- Mental Health, Intellectual and Developmental Disabilities and the Ageing ProcessОт EverandMental Health, Intellectual and Developmental Disabilities and the Ageing ProcessОценок пока нет
- Pharmacology (1) - 104-122Документ19 страницPharmacology (1) - 104-122Dental LecturesMMQОценок пока нет
- Unit 05: Drugs Acting On The Respiratory System Drugs Acting On The Upper Respiratory TractДокумент8 страницUnit 05: Drugs Acting On The Respiratory System Drugs Acting On The Upper Respiratory TractDental LecturesMMQОценок пока нет
- Unit 07: Drugs Acting On The Immune System Anti-Inflammatory, Antiarthritis, and Related AgentsДокумент14 страницUnit 07: Drugs Acting On The Immune System Anti-Inflammatory, Antiarthritis, and Related AgentsDental LecturesMMQОценок пока нет
- Unit 06: Drugs Acting On The Gastrointestinal SystemДокумент9 страницUnit 06: Drugs Acting On The Gastrointestinal SystemDental LecturesMMQОценок пока нет
- Unit 04: Drugs Acting On The Renal System Diuretic Agents: Thiazide and Thiazide-Like DiureticsДокумент8 страницUnit 04: Drugs Acting On The Renal System Diuretic Agents: Thiazide and Thiazide-Like DiureticsDental LecturesMMQОценок пока нет
- Computer Software: Chapter FourДокумент9 страницComputer Software: Chapter FourDental LecturesMMQОценок пока нет
- Unit 03: Drugs Acting On The Cardiovascular System Drugs Affecting Blood PressureДокумент12 страницUnit 03: Drugs Acting On The Cardiovascular System Drugs Affecting Blood PressureDental LecturesMMQОценок пока нет
- Arab American University-Jenin Faculty of Nursing Tel: 04-241-8888, ext.1234 Fax: 04-2510-813:نوفلت 04 - 241 - 8888 ، - 1234 سكاف 04 - 251 - 0813Документ1 страницаArab American University-Jenin Faculty of Nursing Tel: 04-241-8888, ext.1234 Fax: 04-2510-813:نوفلت 04 - 241 - 8888 ، - 1234 سكاف 04 - 251 - 0813Dental LecturesMMQОценок пока нет
- 1 Introduction To Pharmacology: 1.1 BackgroundДокумент10 страниц1 Introduction To Pharmacology: 1.1 BackgroundDental LecturesMMQОценок пока нет
- Drugs Affecting Blood Coagulation: Antiplatelet Agents Therapeutic ActionsДокумент4 страницыDrugs Affecting Blood Coagulation: Antiplatelet Agents Therapeutic ActionsDental LecturesMMQОценок пока нет
- Computer Hardware: Chapter ThreeДокумент28 страницComputer Hardware: Chapter ThreeDental LecturesMMQОценок пока нет
- انغام PDFДокумент5 страницانغام PDFDental LecturesMMQОценок пока нет
- Assignment - 1 - شعبة نمو 7.docx -Документ3 страницыAssignment - 1 - شعبة نمو 7.docx -Dental LecturesMMQОценок пока нет
- Necrosis BasophilsДокумент6 страницNecrosis BasophilsDental LecturesMMQОценок пока нет
- Question1: (3 Points) : Assignment 2 Name: IDДокумент4 страницыQuestion1: (3 Points) : Assignment 2 Name: IDDental LecturesMMQОценок пока нет
- مصطفى توبيك PDFДокумент1 страницаمصطفى توبيك PDFDental LecturesMMQОценок пока нет
- Experiment 4: Chemical Formula of A HydrateДокумент3 страницыExperiment 4: Chemical Formula of A HydrateDental LecturesMMQОценок пока нет
- Experiment 5: The Empirical Formula of Magnesium Oxide: ObjectiveДокумент2 страницыExperiment 5: The Empirical Formula of Magnesium Oxide: ObjectiveDental LecturesMMQОценок пока нет
- Phase State of AV Valves State of Semilunar ValvesДокумент2 страницыPhase State of AV Valves State of Semilunar ValvesDental LecturesMMQОценок пока нет
- Skyscrapers Activities Enjoy Lectures .Costumes .Gift Sculptures Brick Sculptures Pure .DecorateДокумент1 страницаSkyscrapers Activities Enjoy Lectures .Costumes .Gift Sculptures Brick Sculptures Pure .DecorateDental LecturesMMQОценок пока нет
- فندمنتل وظيفة رقم 2Документ2 страницыفندمنتل وظيفة رقم 2Dental LecturesMMQОценок пока нет
- Name: Student ID Number: You Must Show All Your Work To Receive To Full Credit!Документ3 страницыName: Student ID Number: You Must Show All Your Work To Receive To Full Credit!Dental LecturesMMQОценок пока нет
- Biochemistry 1 Lab: Title of The Lab: Use of Pipetmen Andbiochemical CalculationДокумент4 страницыBiochemistry 1 Lab: Title of The Lab: Use of Pipetmen Andbiochemical CalculationDental LecturesMMQОценок пока нет
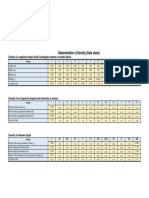
- Experiment 3: Determination of Density: ObjectivesДокумент3 страницыExperiment 3: Determination of Density: ObjectivesDental LecturesMMQОценок пока нет
- Manual Biochemistry-10-2017Документ65 страницManual Biochemistry-10-2017Dental LecturesMMQОценок пока нет
- Data Readings (Groups)Документ1 страницаData Readings (Groups)Dental LecturesMMQОценок пока нет
- Experiment 3: Determination of Density: ObjectivesДокумент3 страницыExperiment 3: Determination of Density: ObjectivesDental LecturesMMQОценок пока нет
- مصطفى توبيكДокумент1 страницаمصطفى توبيكDental LecturesMMQОценок пока нет
- First Question: Student's Name: Adel Sulaiman SectionДокумент5 страницFirst Question: Student's Name: Adel Sulaiman SectionDental LecturesMMQОценок пока нет
- Biology For Medical Science Assignment 2 Name: Adel SulaimanДокумент2 страницыBiology For Medical Science Assignment 2 Name: Adel SulaimanDental LecturesMMQОценок пока нет
- Case Reviews in Ophthalmology Expert Consult - OnlДокумент2 страницыCase Reviews in Ophthalmology Expert Consult - Onldr. mostakОценок пока нет
- AAFP 2015 Proceedings Book For WebДокумент292 страницыAAFP 2015 Proceedings Book For WebPavel VokrouhlíkОценок пока нет
- PuspitaДокумент5 страницPuspitaAjeng NadiaОценок пока нет
- Quality Assurance in NursingДокумент7 страницQuality Assurance in NursingSimran Chauhan100% (1)
- COPARДокумент5 страницCOPARErica Keil MoleОценок пока нет
- Clinical-Psychomotor SkillsДокумент415 страницClinical-Psychomotor SkillsKimG1991100% (2)
- The Hiding Place, by John Burley - ExtractДокумент13 страницThe Hiding Place, by John Burley - ExtractAnonymous ikUR753am100% (1)
- Difficult Airway 2011 Power Point PresentationДокумент54 страницыDifficult Airway 2011 Power Point PresentationBalaji Mallela100% (1)
- Pfizerinc 12557825593101 Phpapp03Документ64 страницыPfizerinc 12557825593101 Phpapp03az2690100% (1)
- TIGER Initiative Informatics DefinitionsДокумент9 страницTIGER Initiative Informatics DefinitionslaggantigganОценок пока нет
- Question Bank: Paper 3 - Organisation of Hospital ServicesДокумент5 страницQuestion Bank: Paper 3 - Organisation of Hospital ServicesDr. Rakshit SolankiОценок пока нет
- Cognitive Behavioral Therapy For Daily Life: Course GuidebookДокумент213 страницCognitive Behavioral Therapy For Daily Life: Course GuidebookZ XN100% (3)
- Admitting and Discharging Patients.Документ15 страницAdmitting and Discharging Patients.FatimaIvanCeniza100% (1)
- Allergy - 2021 - Zuberbier - The International EAACI GA LEN EuroGuiDerm APAAACI Guideline For The DefinitionДокумент33 страницыAllergy - 2021 - Zuberbier - The International EAACI GA LEN EuroGuiDerm APAAACI Guideline For The DefinitionAdelina PopescuОценок пока нет
- Rishum 1 262421216 2Документ1 страницаRishum 1 262421216 2HellcroZОценок пока нет
- Human Factors and NOTSSДокумент31 страницаHuman Factors and NOTSSSunbal MahmoodОценок пока нет
- Commentaries: A New Peritoneal Dialysis Training Guideline From The Ispd Nursing CommitteeДокумент2 страницыCommentaries: A New Peritoneal Dialysis Training Guideline From The Ispd Nursing CommitteeSergio Andres GuerreroОценок пока нет
- An Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Документ66 страницAn Assessment of Manual Medical Record System of Fr. Simpliciano Academy Inc. School Year 2018-2019Dimple SalesОценок пока нет
- Specific Phobias: What Is A Specific Phobia?Документ6 страницSpecific Phobias: What Is A Specific Phobia?Waseem QureshiОценок пока нет
- Roxas Memorial Provincial HospitalДокумент11 страницRoxas Memorial Provincial HospitalJuvie Lie Fancubila FerrenОценок пока нет
- Jurnal MassageДокумент8 страницJurnal MassageDyah PridamiОценок пока нет
- Intro Business Case Analysis PaperДокумент3 страницыIntro Business Case Analysis Paperapi-282833536Оценок пока нет
- Nvoice of Surgical Fees CG Cosmetic Surgery: Robert Hunsaker, M.D Johanna Anzola 8/11/2020 Zuleika BurgosДокумент2 страницыNvoice of Surgical Fees CG Cosmetic Surgery: Robert Hunsaker, M.D Johanna Anzola 8/11/2020 Zuleika BurgoszuleikaОценок пока нет
- Ethical Issues and The ElderlyДокумент15 страницEthical Issues and The Elderlythanuja mathewОценок пока нет
- Kerala CEE PG Ayurveda Admission 2019 Mop Up Counselling On 30.10.2019 Admitted ListДокумент1 страницаKerala CEE PG Ayurveda Admission 2019 Mop Up Counselling On 30.10.2019 Admitted ListSabaОценок пока нет
- HL7 Reference Information ModelДокумент30 страницHL7 Reference Information ModelAgus MutamakinОценок пока нет
- 2 Kanto Region (Kangoshi) Part 2 of 3Документ77 страниц2 Kanto Region (Kangoshi) Part 2 of 3bnp2tkidotgodotid100% (1)
- Professional Development PlanДокумент2 страницыProfessional Development Planapi-245887979100% (1)
- Davao Doctors College, Inc.: Gen. Malvar ST., Davao City College of Allied Health Sciences - Nursing ProgramДокумент20 страницDavao Doctors College, Inc.: Gen. Malvar ST., Davao City College of Allied Health Sciences - Nursing ProgramPRECIOUS DIANNE BARDON-MEMPINОценок пока нет