Вам также может понравиться
- Pengkajian Keperawatan Pada Gangguan THTДокумент35 страницPengkajian Keperawatan Pada Gangguan THTSYAIFULОценок пока нет
- The ENT History and ExaminationДокумент11 страницThe ENT History and ExaminationSuresh MettaОценок пока нет
- Ent Case 2Документ29 страницEnt Case 2Trina CardonaОценок пока нет
- ENT SGD 1 Clinical History and ENT Physical ExaminationДокумент51 страницаENT SGD 1 Clinical History and ENT Physical ExaminationEmerson QuimbaОценок пока нет
- EntДокумент105 страницEntNikhil KumarОценок пока нет
- Ear, Nose and Throat History and ExaminationДокумент7 страницEar, Nose and Throat History and ExaminationStetho Love100% (1)
- Disorders: Their Medical/Surgical Management - Ear: Curriculum M.S. Otolaryngology (ENT)Документ3 страницыDisorders: Their Medical/Surgical Management - Ear: Curriculum M.S. Otolaryngology (ENT)Prasad ReddyОценок пока нет
- ENT Review - Dr. Al SalehДокумент33 страницыENT Review - Dr. Al SalehZuhairSadiqОценок пока нет
- History Taking and Examination of EarДокумент75 страницHistory Taking and Examination of EarShisam PoudelОценок пока нет
- Ent Case Sheet ProformaДокумент8 страницEnt Case Sheet ProformaDebzz Pradhan100% (3)
- Final 641 NodayДокумент9 страницFinal 641 Nodaynatalie nodayОценок пока нет
- Case 12 - A, 25 - Year - Old Student Presents With Bilateral Ear Blockage Associated With Tinnitus. He Has Occasional PainДокумент11 страницCase 12 - A, 25 - Year - Old Student Presents With Bilateral Ear Blockage Associated With Tinnitus. He Has Occasional PainananОценок пока нет
- THEEARДокумент9 страницTHEEARapi-3822433Оценок пока нет
- Approach To Examination of ENT DisordersДокумент39 страницApproach To Examination of ENT DisordersMohammad SaifullahОценок пока нет
- Buku Gejala Pada THTДокумент292 страницыBuku Gejala Pada THTHeldha Nurma SantiОценок пока нет
- ENT Case Proforma-NoseДокумент7 страницENT Case Proforma-NoseGaneshОценок пока нет
- What Is OtolaryngologyДокумент37 страницWhat Is OtolaryngologyPhạm Văn HiệpОценок пока нет
- EntДокумент36 страницEntArya ChoudhuryОценок пока нет
- Otorhinolaryngology Model Paper PGДокумент16 страницOtorhinolaryngology Model Paper PGKanav BaigraОценок пока нет
- Ent DisordersДокумент74 страницыEnt Disorderspslokesha84Оценок пока нет
- Med 1 - 1st Shift - Lec - HEENT Neck ExaminationДокумент3 страницыMed 1 - 1st Shift - Lec - HEENT Neck ExaminationRJLeddaОценок пока нет
- Otolaryngology For Medical StudentsДокумент112 страницOtolaryngology For Medical StudentsDrsreeram ValluriОценок пока нет
- 1b. PENGKAJIAN PENDENGARANДокумент35 страниц1b. PENGKAJIAN PENDENGARANHanip Little-FaqotОценок пока нет
- History Taking and Physical Exam in ENTДокумент75 страницHistory Taking and Physical Exam in ENTSantosh hambardeОценок пока нет
- Acute Otitis MediaДокумент16 страницAcute Otitis Mediaadrianne18sОценок пока нет
- Note On Asthma in AdultДокумент5 страницNote On Asthma in Adultshivam1969Оценок пока нет
- Kuliah Tuli Konduktif Infeksi TelingaДокумент66 страницKuliah Tuli Konduktif Infeksi TelingaRizka Dany AfinaОценок пока нет
- Ent H&PДокумент2 страницыEnt H&Paraagh09Оценок пока нет
- Parts: Nose Throat Pharynx LarynxДокумент47 страницParts: Nose Throat Pharynx LarynxRANJIT GOGOIОценок пока нет
- Infeksi Telinga: Rizka Dany AfinaДокумент63 страницыInfeksi Telinga: Rizka Dany AfinaRizka Dany AfinaОценок пока нет
- Ent For General PracticeДокумент46 страницEnt For General PracticefenixaОценок пока нет
- EntДокумент32 страницыEntaini natasha100% (3)
- Sree's ENT Cognitive AnswersДокумент16 страницSree's ENT Cognitive Answersragulraj6699Оценок пока нет
- Causes of Hearing Loss, Deafness, and Tinnitus/Ringing Ears - Information From NOWiHEAR ProfessionalsДокумент6 страницCauses of Hearing Loss, Deafness, and Tinnitus/Ringing Ears - Information From NOWiHEAR Professionalscheerfulnecessi98Оценок пока нет
- Common ENT Conditions PresentationДокумент60 страницCommon ENT Conditions PresentationMICHAEL SAKALAОценок пока нет
- ENT Case Proforma-EarДокумент8 страницENT Case Proforma-EarGaneshОценок пока нет
- Pediatrics OSCEДокумент28 страницPediatrics OSCEpirate92% (13)
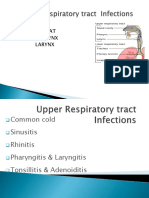
- Upper Airway InfectionsДокумент5 страницUpper Airway InfectionsPhilline MacapagalОценок пока нет
- Case Report OMEДокумент8 страницCase Report OMEYosephine ninaОценок пока нет
- Otitis Media With Effusion: Case ReportДокумент8 страницOtitis Media With Effusion: Case ReportMas KaryonОценок пока нет
- Endodontic Diagnosis and Treatment PlanДокумент89 страницEndodontic Diagnosis and Treatment PlanWasfe BarzaqОценок пока нет
- Catetan BergunaДокумент22 страницыCatetan BergunamellvinОценок пока нет
- SCRUBS Special Teaching Ent Clinical CasesДокумент26 страницSCRUBS Special Teaching Ent Clinical CasesasiyazaidiaОценок пока нет
- Nasal Obstruction: Meng JuanДокумент36 страницNasal Obstruction: Meng JuanReshma VasuОценок пока нет
- OtalgiaДокумент57 страницOtalgiaKamal-Eldin Ahmed Abou-ElhamdОценок пока нет
- Anes History Add OnsДокумент3 страницыAnes History Add OnsDANEKKA TANОценок пока нет
- Anes History Add OnsДокумент3 страницыAnes History Add OnsDANEKKA TANОценок пока нет
- Anes History Add OnsДокумент3 страницыAnes History Add OnsDANEKKA TANОценок пока нет
- Viva Ear For MBBSДокумент7 страницViva Ear For MBBSDr.Riashat azimОценок пока нет
- Concept Map FinaleДокумент31 страницаConcept Map FinaleDeVineОценок пока нет
- Common ENT ComplaintsДокумент9 страницCommon ENT ComplaintsHo Yong WaiОценок пока нет
- Diagnosis of Ent Disorders You Make The CallДокумент137 страницDiagnosis of Ent Disorders You Make The Callsaifsaffa2Оценок пока нет
- 18 Head and NeckДокумент23 страницы18 Head and NeckMahmoud AbuAwadОценок пока нет
- ENT Head and Neck ExamДокумент21 страницаENT Head and Neck ExamvickyОценок пока нет
- Casea Omsk W Fas N PalДокумент28 страницCasea Omsk W Fas N PalMegan ShanzuОценок пока нет
- Test Questions and Answers Near The End: Direct Force Indirect Force Hearing Loss Ringing Bleed OtalgiaДокумент19 страницTest Questions and Answers Near The End: Direct Force Indirect Force Hearing Loss Ringing Bleed OtalgialeeОценок пока нет
- 4 - Assessing EarДокумент7 страниц4 - Assessing EarFrancine Julia MorilloОценок пока нет
- Examination of The Ear, Temporal BoneДокумент1 страницаExamination of The Ear, Temporal BoneRoma Bianca Tan BisdaОценок пока нет
- Case Study Ears 12Документ3 страницыCase Study Ears 12Carla May CaraОценок пока нет
- Otic Preparations: Compounding & Manufacturing II Presentation of Luisabel NoveloДокумент10 страницOtic Preparations: Compounding & Manufacturing II Presentation of Luisabel NoveloNitin SharmaОценок пока нет
- Vestibular Appratus: BY: Harshita YadavДокумент49 страницVestibular Appratus: BY: Harshita YadavNitin SharmaОценок пока нет
- Congenitalinnerearanomalies 160214090056Документ7 страницCongenitalinnerearanomalies 160214090056Nitin SharmaОценок пока нет
- Vestibulo-Ocular Reflex: Asad IqbalДокумент8 страницVestibulo-Ocular Reflex: Asad IqbalNitin SharmaОценок пока нет
- WWW Anatomyqa Com Anatomy Important Question and Answers On Head and Neck Anatomy Posterior Triangle of NeckДокумент15 страницWWW Anatomyqa Com Anatomy Important Question and Answers On Head and Neck Anatomy Posterior Triangle of NeckNitin SharmaОценок пока нет
- Maintaining Balance: The Vestibular SystemДокумент28 страницMaintaining Balance: The Vestibular SystemMohammad Farouq OmarОценок пока нет
- Complication of Neck Dissection & Its Management.: Dr. Sanjay Maharjan 1 Yr Resident, Ent-Hns, MTH, PokharaДокумент37 страницComplication of Neck Dissection & Its Management.: Dr. Sanjay Maharjan 1 Yr Resident, Ent-Hns, MTH, PokharaNitin SharmaОценок пока нет
- Deep Cervical Fascia - Investing Layer - Prevertebral Layer - Pretracheal Layer - Carotid Sheath - AnatomyQAДокумент9 страницDeep Cervical Fascia - Investing Layer - Prevertebral Layer - Pretracheal Layer - Carotid Sheath - AnatomyQANitin SharmaОценок пока нет
- Complication of Neck Dissection & Its Management.: Dr. Sanjay Maharjan 1 Yr Resident, Ent-Hns, MTH, PokharaДокумент37 страницComplication of Neck Dissection & Its Management.: Dr. Sanjay Maharjan 1 Yr Resident, Ent-Hns, MTH, PokharaNitin SharmaОценок пока нет
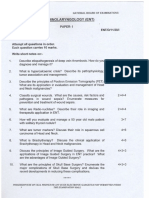
- Otorhinolaryngology (Ent) Dec11Документ4 страницыOtorhinolaryngology (Ent) Dec11Nitin SharmaОценок пока нет
- Deep Cervical Fascia - Investing Layer - Prevertebral Layer - Pretracheal Layer - Carotid Sheath - AnatomyQAДокумент9 страницDeep Cervical Fascia - Investing Layer - Prevertebral Layer - Pretracheal Layer - Carotid Sheath - AnatomyQANitin SharmaОценок пока нет
- Ent - DEC 2010 PDFДокумент4 страницыEnt - DEC 2010 PDFjerinthomasrajanОценок пока нет
- Congenitalinnerearanomalies 160214090056Документ7 страницCongenitalinnerearanomalies 160214090056Nitin SharmaОценок пока нет
- Assessment of HearingДокумент30 страницAssessment of HearingNitin SharmaОценок пока нет
- GRBASДокумент4 страницыGRBASNitin Sharma100% (1)
- Diseasesofexternalear 1Документ86 страницDiseasesofexternalear 1Nitin Sharma100% (1)
- Audiology: DR Humra ShamimДокумент69 страницAudiology: DR Humra ShamimNitin SharmaОценок пока нет
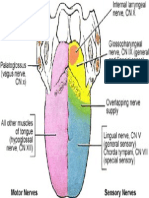
- 02 Tongue Innervation 288x430Документ1 страница02 Tongue Innervation 288x430Nitin SharmaОценок пока нет
- Oral LesionsДокумент4 страницыOral LesionsNitin SharmaОценок пока нет
- AssessmentofhearingДокумент85 страницAssessmentofhearingNitin SharmaОценок пока нет
- Pta SymbolsДокумент1 страницаPta SymbolsNitin SharmaОценок пока нет
- Grbas ScaleДокумент1 страницаGrbas ScaleNitin SharmaОценок пока нет
- Society of Nuclear Medicine Procedure Guideline For Thyroid ScintigraphyДокумент4 страницыSociety of Nuclear Medicine Procedure Guideline For Thyroid Scintigraphyahmedmaksoud2036Оценок пока нет
- Radiation Safety and AlaraДокумент2 страницыRadiation Safety and AlarawesmorangaОценок пока нет
- Anatomy of Paranasal SinusesДокумент49 страницAnatomy of Paranasal SinusesNitin SharmaОценок пока нет
- Treacher Colli SyndromeДокумент25 страницTreacher Colli SyndromeNitin Sharma100% (1)
- WWW Asha OrgДокумент7 страницWWW Asha OrgNitin SharmaОценок пока нет
- DD of Hearing LossДокумент1 страницаDD of Hearing LossNitin SharmaОценок пока нет
- Branchial Pharyngeal Arches ConciseДокумент66 страницBranchial Pharyngeal Arches ConciseRitika Ahuja MalhotraОценок пока нет
- Midterm Exam Structure of EnglishДокумент2 страницыMidterm Exam Structure of EnglishReñer Aquino BystanderОценок пока нет
- Urinary Tract Infection Among First Year BMLS Student of SMUДокумент4 страницыUrinary Tract Infection Among First Year BMLS Student of SMUJunfel ZablanОценок пока нет
- TELEMEDICINEДокумент2 страницыTELEMEDICINESILLA ELSA SOJIОценок пока нет
- 166-176 The Role of Financial Behavior in Mediation The Influence of Financial Literacy and Financial Self Efficacy On Financial Will BeingДокумент11 страниц166-176 The Role of Financial Behavior in Mediation The Influence of Financial Literacy and Financial Self Efficacy On Financial Will BeingJuvy ParaguyaОценок пока нет
- Prawira Yuda Husada - 211810532Документ8 страницPrawira Yuda Husada - 211810532Yuda HusadaОценок пока нет
- I. Choose A, B, C or D That Has The Underlined Part Pronounced DifferentlyДокумент5 страницI. Choose A, B, C or D That Has The Underlined Part Pronounced DifferentlyHà Giang Nguyễn ThịОценок пока нет
- WN.74. Akira Annaisha - Case Notes - Acute Meningoencephalitis - Writing - Nursing - OETДокумент3 страницыWN.74. Akira Annaisha - Case Notes - Acute Meningoencephalitis - Writing - Nursing - OETmk1971953Оценок пока нет
- Understanding Technology Use Throughout Development What Erik Erikson Would Say About Toddler Tweets and Facebook FriendsДокумент11 страницUnderstanding Technology Use Throughout Development What Erik Erikson Would Say About Toddler Tweets and Facebook FriendselaineОценок пока нет
- Group A: Private Entities/Sector:: San Miguel Foods, IncДокумент8 страницGroup A: Private Entities/Sector:: San Miguel Foods, IncRio AlbaricoОценок пока нет
- QR Scientifique Technique EN 011119Документ29 страницQR Scientifique Technique EN 011119Vio CondreiОценок пока нет
- The Compound Effect Changing HabitsДокумент4 страницыThe Compound Effect Changing HabitsYash TyagiОценок пока нет
- Extraction of Kissing Molars With Tooth Sectioning TechniqueДокумент5 страницExtraction of Kissing Molars With Tooth Sectioning Techniquekiara wardanaОценок пока нет
- Cpe Practice Tests 1Документ32 страницыCpe Practice Tests 1garaziskills100% (2)
- Renal 2005 Exam QuestionsДокумент34 страницыRenal 2005 Exam QuestionsnarasimhahanОценок пока нет
- SHS Health Optimizing Physical Education 4Документ4 страницыSHS Health Optimizing Physical Education 4Jennifer A. IñigoОценок пока нет
- Test OgenДокумент65 страницTest OgenMichael PogodaОценок пока нет
- Tle - H.E. - Housekeeping: Quarter 2 - Module 1: Select and Set Up Equipment and MaterialsДокумент24 страницыTle - H.E. - Housekeeping: Quarter 2 - Module 1: Select and Set Up Equipment and MaterialsRonaldo Oloroso Abinal Jr.Оценок пока нет
- Ramanlal P. Patel Word-Index With Rubrics of Kent's RepertoryДокумент9 страницRamanlal P. Patel Word-Index With Rubrics of Kent's Repertorynaveen kumar100% (1)
- Hispanic Caregivers Beliefs and Perceptions of Early Childhood CariesДокумент12 страницHispanic Caregivers Beliefs and Perceptions of Early Childhood Cariesapi-597791259Оценок пока нет
- REFERENCESДокумент5 страницREFERENCESKrista. metersОценок пока нет
- OB Case StudyДокумент52 страницыOB Case StudyMaria ThereseОценок пока нет
- Vitamina E HPLC - Grupa 24Документ5 страницVitamina E HPLC - Grupa 24Daniela PopaОценок пока нет
- 1.2.2.5 Lab - What Was TakenДокумент2 страницы1.2.2.5 Lab - What Was TakenPhillip NguyenОценок пока нет
- CR Muhammad Arif Ardiansyah Tugas BingДокумент4 страницыCR Muhammad Arif Ardiansyah Tugas BingMUHAMMAD ARIF ARDIANSYAHОценок пока нет
- Types of Simulation in Nursing EducationДокумент7 страницTypes of Simulation in Nursing EducationKarl RobleОценок пока нет
- The Humorous Rewriting of Orwells 1984 The GreekДокумент16 страницThe Humorous Rewriting of Orwells 1984 The GreeknuriaОценок пока нет
- Resume and Cover Letter-Addison Malcolm 1Документ3 страницыResume and Cover Letter-Addison Malcolm 1api-547229642Оценок пока нет
- News Item TextДокумент3 страницыNews Item TextMiftahus salamahОценок пока нет
- CARDIOLABS ICU Ventilator For Adult & Pediatric Online - GeM - 950000Документ10 страницCARDIOLABS ICU Ventilator For Adult & Pediatric Online - GeM - 950000chandan kumarОценок пока нет
- The Russian Girl - Melissa NДокумент205 страницThe Russian Girl - Melissa NphlayersОценок пока нет