Вам также может понравиться
- Sas of DR Prashant ShahДокумент2 страницыSas of DR Prashant Shahsrijan consultancyОценок пока нет
- Sas of DR Mohan C. RegmiДокумент2 страницыSas of DR Mohan C. Regmisrijan consultancyОценок пока нет
- Spektra-PN FormatДокумент3 страницыSpektra-PN FormatRahul JainОценок пока нет
- 7-A - 0T-Px5r-: Government of Odisha Health & Family Welfare Department OrderДокумент1 страница7-A - 0T-Px5r-: Government of Odisha Health & Family Welfare Department OrderUpasana PattnaikОценок пока нет
- Ii., 9. O3. Zoi 9: Government of Odisha Health & Family Welfare Department Order No. 6Документ2 страницыIi., 9. O3. Zoi 9: Government of Odisha Health & Family Welfare Department Order No. 6Soumyaranjan BeheraОценок пока нет
- AJQBG7 LForm 1 AfinalДокумент35 страницAJQBG7 LForm 1 AfinalNandini JanpageОценок пока нет
- Note: Vacancies May Be Increased/decreasedДокумент3 страницыNote: Vacancies May Be Increased/decreasedvinay reddyОценок пока нет
- Chemical For Scale InhibitorДокумент401 страницаChemical For Scale InhibitorSaras Unggul Utami100% (1)
- Coimbatore Thiruppur EmpДокумент4 страницыCoimbatore Thiruppur Emppriya selvarajОценок пока нет
- Adobe Scan 12 Apr 2023Документ2 страницыAdobe Scan 12 Apr 2023Sashil ReddyОценок пока нет
- Cghs Room RentДокумент4 страницыCghs Room RentaosalaryjlОценок пока нет
- RFQ#08-1043 Airconditioning SystemДокумент1 страницаRFQ#08-1043 Airconditioning Systemerosennin2006Оценок пока нет
- causelistALL2022 08 25 2Документ160 страницcauselistALL2022 08 25 2Akash TandonОценок пока нет
- Personal Form For Professional IndemnityДокумент1 страницаPersonal Form For Professional IndemnityLilammani ChapagainОценок пока нет
- Notice - FinalДокумент2 страницыNotice - FinalPrabir Kumar ChatterjeeОценок пока нет
- Mamc Ortho PG Course 2019Документ2 страницыMamc Ortho PG Course 2019Pankaj VatsaОценок пока нет
- Expenses Resign Reza 2018Документ8 страницExpenses Resign Reza 2018H1H010034Оценок пока нет
- Vims 25092019 PDFДокумент4 страницыVims 25092019 PDFVasanth Kumar AllaОценок пока нет
- Exp EstimateДокумент1 страницаExp EstimatenelsngОценок пока нет
- Oil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisДокумент3 страницыOil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisAbhinav KumarОценок пока нет
- causelistALL2021 10 25Документ129 страницcauselistALL2021 10 25Aksharva HomesОценок пока нет
- Validity of CGHS Card in All Wellness Centres OM Dated 1st May 2023Документ2 страницыValidity of CGHS Card in All Wellness Centres OM Dated 1st May 2023Dilawar Singh YadavОценок пока нет
- Application Form RBI Bank Medical Consultant PostsДокумент2 страницыApplication Form RBI Bank Medical Consultant PostsNeha SharmaОценок пока нет
- B.S. N. L.: Hassan TДокумент10 страницB.S. N. L.: Hassan TEBОценок пока нет
- DR Raju KadamДокумент4 страницыDR Raju KadamMagathaОценок пока нет
- causelistALL2022 08 31 2Документ114 страницcauselistALL2022 08 31 2Akash TandonОценок пока нет
- Notification: Andhra Medical DistrictДокумент9 страницNotification: Andhra Medical Districtthambisetty prudhviОценок пока нет
- MemoДокумент18 страницMemoAsad ZahidiОценок пока нет
- causelistALL2022 08 29Документ174 страницыcauselistALL2022 08 29Akash TandonОценок пока нет
- PBR Proposal TemplateДокумент10 страницPBR Proposal TemplatePraveen KumarОценок пока нет
- Privi Data SheetДокумент416 страницPrivi Data SheetKunalGopalAgiwaleОценок пока нет
- Birthing Homes ReqДокумент10 страницBirthing Homes ReqMi Lagro100% (2)
- Cash Advance MAP Q1 2023 JoPДокумент13 страницCash Advance MAP Q1 2023 JoPArfan ArifinОценок пока нет
- Advertizement 2Документ3 страницыAdvertizement 2drrajkharshОценок пока нет
- 2009 DetailsДокумент19 страниц2009 DetailshrrcrgkОценок пока нет
- Deputation of OMHScadre PDFДокумент2 страницыDeputation of OMHScadre PDFAnamika DasОценок пока нет
- Letter For Demanding Arrears of Approved Msbte StaffДокумент5 страницLetter For Demanding Arrears of Approved Msbte StaffDIPAK VINAYAK SHIRBHATEОценок пока нет
- 233 - Petrol Expense of Outreach Executive Oct To Dec - Rahil DesaiДокумент1 страница233 - Petrol Expense of Outreach Executive Oct To Dec - Rahil DesaiGokulОценок пока нет
- Barangay Drug Clearing Program: Checklists, Certifications and Other FORMSДокумент18 страницBarangay Drug Clearing Program: Checklists, Certifications and Other FORMSBcpo Naguilian RoadОценок пока нет
- Bhimasakha ExecutiveДокумент18 страницBhimasakha ExecutiveAdvocate Annu KrishnaОценок пока нет
- Paramedical CouncilДокумент2 страницыParamedical CouncilSachin kumarОценок пока нет
- DR List Mharashtra MBBS MOДокумент27 страницDR List Mharashtra MBBS MOVAIBHAV P ANPAT100% (1)
- DO. Rc. No.96-NUHM-HWC-2017.Документ10 страницDO. Rc. No.96-NUHM-HWC-2017.swapnitha tummaОценок пока нет
- Assam Doctors ListДокумент31 страницаAssam Doctors ListDivya TanejaОценок пока нет
- Federal Staff Relief Fund FormДокумент1 страницаFederal Staff Relief Fund Formkazmi_jeОценок пока нет
- Hvs PDFДокумент6 страницHvs PDFRajnishОценок пока нет
- Causelist12024 03 06Документ17 страницCauselist12024 03 06td4wnzp469Оценок пока нет
- Avid Organics VRD Eia1 PDFДокумент133 страницыAvid Organics VRD Eia1 PDFmehul10941Оценок пока нет
- Dental ProformaДокумент2 страницыDental ProformaEhsin AliОценок пока нет
- Medical Reimbursement Dipika Vasava 2019-20Документ2 страницыMedical Reimbursement Dipika Vasava 2019-20praful2604Оценок пока нет
- Hosneara Begum - Aastha ConcentДокумент2 страницыHosneara Begum - Aastha ConcentAbul HasnatОценок пока нет
- Travelling Application: B.Braun Medical Indonesia. PTДокумент7 страницTravelling Application: B.Braun Medical Indonesia. PTbali nusraОценок пока нет
- causelistALL2022 08 31Документ112 страницcauselistALL2022 08 31Akash TandonОценок пока нет
- Tour Programme: Twilight Litaka Pharma LTDДокумент5 страницTour Programme: Twilight Litaka Pharma LTDJagadeesh Hm HmОценок пока нет
- Sl. No. Name of Drugs/medical Device/cosmetics Batch No./Date of Manufacture/Date of Expiry/Manufactured by Reason For Failure Drawn by FromДокумент6 страницSl. No. Name of Drugs/medical Device/cosmetics Batch No./Date of Manufacture/Date of Expiry/Manufactured by Reason For Failure Drawn by FromDeepak MoryaОценок пока нет
- SPJ Perawatan BerangasДокумент12 страницSPJ Perawatan BerangasazwarОценок пока нет
- G.O.102 PensionersДокумент3 страницыG.O.102 PensionersNarasimha SastryОценок пока нет
- Workshop Submission PerformaДокумент4 страницыWorkshop Submission PerformaHimanshu GoelОценок пока нет
- causelistALL2021 11 22Документ177 страницcauselistALL2021 11 22nalin soodОценок пока нет
- ATCURON & ADENOJECT PROJ. - BiplawДокумент2 страницыATCURON & ADENOJECT PROJ. - Biplawsrijan consultancyОценок пока нет
- Anaesthesia JR List BiplawДокумент2 страницыAnaesthesia JR List Biplawsrijan consultancyОценок пока нет
- Anaesthesia Doctor List: Locality SC Code DR Name QualificationДокумент2 страницыAnaesthesia Doctor List: Locality SC Code DR Name Qualificationsrijan consultancyОценок пока нет
- Appraisal Form - ExcerptДокумент1 страницаAppraisal Form - Excerptsrijan consultancyОценок пока нет
- Anesth Investment 2012-13 To 2014-15 BiplawДокумент2 страницыAnesth Investment 2012-13 To 2014-15 Biplawsrijan consultancyОценок пока нет
- 100 Chemist List BiplawДокумент9 страниц100 Chemist List Biplawsrijan consultancyОценок пока нет
- Make A Difference With An Australia Awards ScholarshipДокумент8 страницMake A Difference With An Australia Awards Scholarshipsrijan consultancyОценок пока нет
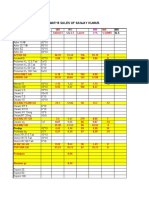
- YTD Sales March'15Документ32 страницыYTD Sales March'15srijan consultancyОценок пока нет
- Balance To Do'14-15 BiplawДокумент2 страницыBalance To Do'14-15 Biplawsrijan consultancyОценок пока нет
- Australia Awards Scholarship Application FormДокумент20 страницAustralia Awards Scholarship Application Formsrijan consultancyОценок пока нет
- Top 5 YTD Mar'15 BiplawДокумент1 страницаTop 5 YTD Mar'15 Biplawsrijan consultancyОценок пока нет
- Nomination Form For Government of Nepal Nominees For Australia Awards Scholarships Intake 2016 Important NotesДокумент3 страницыNomination Form For Government of Nepal Nominees For Australia Awards Scholarships Intake 2016 Important Notessrijan consultancyОценок пока нет
- English Language RequirementsДокумент1 страницаEnglish Language Requirementssrijan consultancyОценок пока нет
- Demand and Supply Chapte RДокумент38 страницDemand and Supply Chapte Rsrijan consultancyОценок пока нет
- Nepal: Applying For An Australia Awards ScholarshipДокумент4 страницыNepal: Applying For An Australia Awards Scholarshipsrijan consultancyОценок пока нет
- Unit-6 National IncomeДокумент51 страницаUnit-6 National Incomesrijan consultancyОценок пока нет
- Australia Awards Scholarship Application FormДокумент20 страницAustralia Awards Scholarship Application Formsrijan consultancyОценок пока нет
- Unit-6 National IncomeДокумент51 страницаUnit-6 National Incomesrijan consultancyОценок пока нет
- Australia Awards Scholarship Application FormДокумент20 страницAustralia Awards Scholarship Application Formsrijan consultancyОценок пока нет
- Demand and Supply Chapte RДокумент38 страницDemand and Supply Chapte Rsrijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Concepts of Cost & Various Types of Cost: UNIT-4Документ22 страницыConcepts of Cost & Various Types of Cost: UNIT-4srijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Traded Companies No. of Transactions Max Price Min Price Closing PriceДокумент2 страницыTraded Companies No. of Transactions Max Price Min Price Closing Pricesrijan consultancyОценок пока нет
- Pentacon Six-02Документ28 страницPentacon Six-02Melissa Moreira TYОценок пока нет
- JAR Part 66 Examination Mod 03Документ126 страницJAR Part 66 Examination Mod 03Shreyas PingeОценок пока нет
- 13 Methods To Increase Your Conditioning - Strength by SkylerДокумент5 страниц13 Methods To Increase Your Conditioning - Strength by SkylerMarko Štambuk100% (1)
- 20BCEC1109, 20BCE1170, 20BCE1233 - IOT Final ReportДокумент40 страниц20BCEC1109, 20BCE1170, 20BCE1233 - IOT Final Reportharsh chauhanОценок пока нет
- Aits 2324 Ot I Jeea TD Paper 2 OfflineДокумент14 страницAits 2324 Ot I Jeea TD Paper 2 OfflineAshish SharmaОценок пока нет
- Mrunal Handout 12 CSP20Документ84 страницыMrunal Handout 12 CSP20SREEKANTHОценок пока нет
- InfertilityДокумент8 страницInfertilityrivannyОценок пока нет
- Canfield FairДокумент3 страницыCanfield Fairapi-546463844Оценок пока нет
- Dysfunctional Uterine Bleeding (DUB)Документ1 страницаDysfunctional Uterine Bleeding (DUB)Bheru LalОценок пока нет
- 2012 U.S. History End-of-Course (EOC) Assessment Field Test Fact SheetДокумент2 страницы2012 U.S. History End-of-Course (EOC) Assessment Field Test Fact SheetswainanjanОценок пока нет
- T103 InstructionsДокумент1 страницаT103 Instructionsjtcool74Оценок пока нет
- The Allied Valve Spares Manufacturer Company Maharashtra IndiaДокумент10 страницThe Allied Valve Spares Manufacturer Company Maharashtra IndiaThe Allied Valve Spares Manufacturer CompanyОценок пока нет
- Northbrook CollegeДокумент10 страницNorthbrook CollegeDaniyal AsifОценок пока нет
- Ivon Neil Adams Form IV RedactedДокумент3 страницыIvon Neil Adams Form IV Redactedkc wildmoonОценок пока нет
- The Importance of Early Childhood InterventionДокумент11 страницThe Importance of Early Childhood Interventionsilverlining0814100% (3)
- ReclosersДокумент28 страницReclosersSteven BeharryОценок пока нет
- Gambaran Professional Quality of Life Proqol GuruДокумент7 страницGambaran Professional Quality of Life Proqol Gurufebrian rahmatОценок пока нет
- Work Environment Act (1977:1160) : Chapter 1 Purpose and Scope of The ActДокумент26 страницWork Environment Act (1977:1160) : Chapter 1 Purpose and Scope of The ActNatalie BlackmoreОценок пока нет
- Amino AcidsДокумент17 страницAmino AcidsSiddharth Rohilla100% (2)
- Anti-Bribery and Corruption PolicyДокумент2 страницыAnti-Bribery and Corruption PolicyAJAY PatilОценок пока нет
- Public Speaking ScriptДокумент2 страницыPublic Speaking ScriptDhia MizaОценок пока нет
- Msds SilverДокумент5 страницMsds SilverSteppenwolf2012Оценок пока нет
- Here's HowДокумент2 страницыHere's HowEden Dela CruzОценок пока нет
- Culturally Safe Classroom Context PDFДокумент2 страницыCulturally Safe Classroom Context PDFdcleveland1706Оценок пока нет
- Dirty Dozen List of Endocrine DisruptorsДокумент4 страницыDirty Dozen List of Endocrine DisruptorsMariuszОценок пока нет
- Case Analysis: Beth OwensДокумент8 страницCase Analysis: Beth OwensPhillip CookОценок пока нет
- Concrete and Its PropertiesДокумент24 страницыConcrete and Its PropertiesAmila LiyanaarachchiОценок пока нет
- Science Form 3 2020 (Notes, PBD, Exercise) : Chapter: 8 RadioactivityДокумент19 страницScience Form 3 2020 (Notes, PBD, Exercise) : Chapter: 8 Radioactivitysakinah100% (1)
- Employee Leave PolicyДокумент3 страницыEmployee Leave Policyladdu30Оценок пока нет
- Red Bank Squadron - 01/22/1942Документ28 страницRed Bank Squadron - 01/22/1942CAP History LibraryОценок пока нет