Вам также может понравиться
- Complete Electronics Self-Teaching Guide with ProjectsОт EverandComplete Electronics Self-Teaching Guide with ProjectsРейтинг: 3 из 5 звезд3/5 (2)
- Basic Electricity Is Described in Many Ways. When AnДокумент6 страницBasic Electricity Is Described in Many Ways. When AnJasonKoylassОценок пока нет
- Rme April 2019 Exam 7 Key PDFДокумент8 страницRme April 2019 Exam 7 Key PDFJevan CalaqueОценок пока нет
- Basic Concepts of ElectronicsДокумент7 страницBasic Concepts of ElectronicsmackoypogiОценок пока нет
- Grade 11 Physics ModuleДокумент119 страницGrade 11 Physics ModuleJoanne Moh100% (1)
- Student Lab Manual: Fundamentals of ElectricityДокумент9 страницStudent Lab Manual: Fundamentals of ElectricityAbdisalam A. MohamedОценок пока нет
- Basic Electricity ParametersДокумент90 страницBasic Electricity Parameterssubbaiah54100% (1)
- China TV Repair HistoryДокумент22 страницыChina TV Repair Historynelson/igan100% (3)
- Short Circuit CalculationsДокумент10 страницShort Circuit CalculationsvenkateshbitraОценок пока нет
- IGCSE 23 Current&VoltageInCircuitsДокумент32 страницыIGCSE 23 Current&VoltageInCircuitsSam JordanОценок пока нет
- Project Report: Topic:-Portable Mobile ChargerДокумент15 страницProject Report: Topic:-Portable Mobile ChargerrohitkgangotiaОценок пока нет
- Avo All Wave Avo-OscillatorДокумент7 страницAvo All Wave Avo-OscillatorPeter Moss100% (1)
- Lecture 4 - BUILDING UTILITIES - Electrical SystemДокумент116 страницLecture 4 - BUILDING UTILITIES - Electrical Systemjona serranoОценок пока нет
- Intro-Duction To Electricity: Force Field Which Is Neither Gravitational Nor Nuclear. To Understand What ThisДокумент9 страницIntro-Duction To Electricity: Force Field Which Is Neither Gravitational Nor Nuclear. To Understand What ThisAbdisalam A. MohamedОценок пока нет
- Voltage: CurrentДокумент21 страницаVoltage: CurrentHeidi RiegoОценок пока нет
- Chapter 9 PLCCДокумент26 страницChapter 9 PLCCpruddviОценок пока нет
- Mod. 1 Basic ElectricalДокумент21 страницаMod. 1 Basic Electricalderping lemon100% (1)
- Biophysics Basics in ElectrotherapyДокумент31 страницаBiophysics Basics in ElectrotherapyrabeyaОценок пока нет
- Schneider MV Design Guide Switchgear DefinitionДокумент21 страницаSchneider MV Design Guide Switchgear DefinitionAdemEfeОценок пока нет
- Solution Manual For Electronic Principles 8th Edition by Malvino Chapters 1 22 PDFДокумент6 страницSolution Manual For Electronic Principles 8th Edition by Malvino Chapters 1 22 PDFWaseem Hassan13% (16)
- Electrical FundamentalsДокумент21 страницаElectrical FundamentalsBWUBPT20024 AVIK MAJIОценок пока нет
- Ge2151 Beee NotesДокумент143 страницыGe2151 Beee NotesNanda Subramanian100% (1)
- Electrotherapy AllДокумент342 страницыElectrotherapy Allbikedet268Оценок пока нет
- Electrical CurrentsДокумент66 страницElectrical Currentsbikedet268Оценок пока нет
- Basic ElectricityДокумент19 страницBasic ElectricityTerfaia NadjatОценок пока нет
- UNIT I NotesДокумент34 страницыUNIT I NotesKarthikeyan VОценок пока нет
- Iii. Internet Related Electric CurrentДокумент25 страницIii. Internet Related Electric CurrentDexterОценок пока нет
- Unit-1 2Документ20 страницUnit-1 2Akhilesh Kumar MishraОценок пока нет
- Electronics Reveiwer WieeДокумент15 страницElectronics Reveiwer Wieejeidre pamorcaОценок пока нет
- DC CircuitsДокумент26 страницDC CircuitsMary Jean ParagsaОценок пока нет
- 276 - BE8251 Basic Electrical and Electronics Engineering - UNIT I ELECTRICAL CIRCUITS and MEASUREMENTS NotesДокумент42 страницы276 - BE8251 Basic Electrical and Electronics Engineering - UNIT I ELECTRICAL CIRCUITS and MEASUREMENTS NotesBalaОценок пока нет
- BEEEДокумент145 страницBEEERohith GajawadaОценок пока нет
- Self InductДокумент22 страницыSelf Inductsiva balanОценок пока нет
- Physics ProjectДокумент22 страницыPhysics ProjectthaswikaamaraОценок пока нет
- Ee00 PPPДокумент203 страницыEe00 PPPlunalight253Оценок пока нет
- E3 Electric Current !: ObjectivesДокумент14 страницE3 Electric Current !: Objectivesostojic007Оценок пока нет
- 1-Introduction To Electrical Current in Physical Therapy201718-1Документ49 страниц1-Introduction To Electrical Current in Physical Therapy201718-1robertОценок пока нет
- Electrical CurrentДокумент28 страницElectrical Currentmanjari guptaОценок пока нет
- Trabajo Guia InglishДокумент10 страницTrabajo Guia InglishAlejandroDuranОценок пока нет
- Electrical Circuits - Learning OutcomesДокумент10 страницElectrical Circuits - Learning OutcomesonaaaaangОценок пока нет
- Jose RizalДокумент11 страницJose RizalBaet RayanОценок пока нет
- Electric Charge:: EL-101 Basic ElectronicsДокумент12 страницElectric Charge:: EL-101 Basic ElectronicsMuhammad Azeem Raza ShahОценок пока нет
- Chapter 1 - Elements of Electrical Circuits PDFДокумент8 страницChapter 1 - Elements of Electrical Circuits PDFAlfred Wong Yi ZhengОценок пока нет
- AbstractДокумент9 страницAbstractSimranОценок пока нет
- Practico-Parcial Eletronica PDFДокумент4 страницыPractico-Parcial Eletronica PDFAlan MamaniОценок пока нет
- The Basics of Electricity CompleteДокумент9 страницThe Basics of Electricity CompleteAlejandroDuranОценок пока нет
- AC: An Electric Current That Continually Reverses DirectionДокумент3 страницыAC: An Electric Current That Continually Reverses DirectionYveth MacionОценок пока нет
- New AQA ELC Science Component 6: Electricity, Magnetism and WavesДокумент2 страницыNew AQA ELC Science Component 6: Electricity, Magnetism and WavesChris HarrisОценок пока нет
- BasicДокумент20 страницBasicG Sandeep KumarОценок пока нет
- Physics Project (Investigatory Project 9)Документ8 страницPhysics Project (Investigatory Project 9)Ashu58% (19)
- ElectricalДокумент26 страницElectrical3re0oooОценок пока нет
- Module 3: Electrical Circuits: On Completion of This Module, You Will Be Able ToДокумент11 страницModule 3: Electrical Circuits: On Completion of This Module, You Will Be Able ToMustapha IsaadОценок пока нет
- Electric Current Means, Depending On The Context, A Flow ofДокумент9 страницElectric Current Means, Depending On The Context, A Flow ofClai GarciaОценок пока нет
- 2 Basic ElectricityДокумент5 страниц2 Basic Electricityfaheem ahmedОценок пока нет
- Grade 9 IctДокумент18 страницGrade 9 IctJohn Carl ToledoОценок пока нет
- Electric Current 11-07-08Документ6 страницElectric Current 11-07-08api-3746683Оценок пока нет
- Module 1 (The Electric Circuits)Документ11 страницModule 1 (The Electric Circuits)Xavier Vincent VisayaОценок пока нет
- Basics of ElectricityДокумент9 страницBasics of ElectricityMelkin NPОценок пока нет
- Hm's Law EquationДокумент4 страницыHm's Law EquationRavi KumarОценок пока нет
- Electric Current 10Документ17 страницElectric Current 10matttttmatteОценок пока нет
- EMF (Electromagnetic) Pollution and RemediationДокумент53 страницыEMF (Electromagnetic) Pollution and RemediationEcopolitan - your Eco-Health Network100% (3)
- Self Inductance of A CoilДокумент8 страницSelf Inductance of A CoilUnknown RiderОценок пока нет
- 1.8electricity For Welding 1.8.1principles of Electricity - Arc Welding Is A Method of Joining Metals Accomplished by ApplyingДокумент1 страница1.8electricity For Welding 1.8.1principles of Electricity - Arc Welding Is A Method of Joining Metals Accomplished by ApplyingLixam NegroОценок пока нет
- Concept of Current:: Electrical EngineeringДокумент7 страницConcept of Current:: Electrical EngineeringRam VigneshОценок пока нет
- Electromagnetic InductionДокумент8 страницElectromagnetic InductionSanjay GuptaОценок пока нет
- OhmДокумент3 страницыOhmJay Ann PanganОценок пока нет
- Iitm Diploma 1st Year FeeeДокумент62 страницыIitm Diploma 1st Year Feeeblackgoku1512007Оценок пока нет
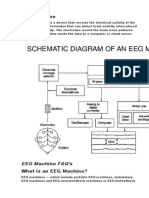
- EEG MachineДокумент3 страницыEEG MachineOlea ScorpanОценок пока нет
- Suture MaterialДокумент76 страницSuture MaterialOlea ScorpanОценок пока нет
- Working Principle of Biosensors: Respiratory System Renal SystemДокумент2 страницыWorking Principle of Biosensors: Respiratory System Renal SystemOlea ScorpanОценок пока нет
- Neuropatia SciaticaДокумент2 страницыNeuropatia SciaticaOlea ScorpanОценок пока нет
- Bio InstrumentationДокумент15 страницBio InstrumentationOlea ScorpanОценок пока нет
- The Portal Vein, The Main Blood Supply To The Liver. Clear Evidence That Cells Delivered Via TheДокумент4 страницыThe Portal Vein, The Main Blood Supply To The Liver. Clear Evidence That Cells Delivered Via TheOlea ScorpanОценок пока нет
- Zhongguo Zhen JiuДокумент2 страницыZhongguo Zhen JiuOlea ScorpanОценок пока нет
- 1472 6963 10 213 2Документ10 страниц1472 6963 10 213 2Olea ScorpanОценок пока нет
- Facial Nerve Palsy: Original Article Contributed byДокумент8 страницFacial Nerve Palsy: Original Article Contributed byOlea ScorpanОценок пока нет
- DDR Memory Termination Regulator With Standby Mode and Enhanced EfficiencyДокумент16 страницDDR Memory Termination Regulator With Standby Mode and Enhanced EfficiencyIslam RabieОценок пока нет
- Monroe Surface Resistivity Meter 292Документ9 страницMonroe Surface Resistivity Meter 292GuillermoОценок пока нет
- Current ElecДокумент56 страницCurrent Elecsuresh_tОценок пока нет
- Technical Specification 2xy CableДокумент13 страницTechnical Specification 2xy CablejamilОценок пока нет
- Standardised Training ManualДокумент98 страницStandardised Training Manualm100% (1)
- EE104xДокумент77 страницEE104xJeff CayetanoОценок пока нет
- Esm Bank Soal Sma 2 (English)Документ25 страницEsm Bank Soal Sma 2 (English)mayang segaraОценок пока нет
- Task 1 P1, M1, D1 Unit17Документ6 страницTask 1 P1, M1, D1 Unit17Hasan Ahmed0% (1)
- MCQs of BHY (22102) Sem-IДокумент43 страницыMCQs of BHY (22102) Sem-ISandesh DalviОценок пока нет
- Alternating Current PDFДокумент18 страницAlternating Current PDFVishwa MoteОценок пока нет
- Types of DC Motors: From The Above Circuit Diagram We Have The Current Relation AsДокумент3 страницыTypes of DC Motors: From The Above Circuit Diagram We Have The Current Relation AsAishwaryaОценок пока нет
- Topic 1 Basic Concept of ElectricityДокумент38 страницTopic 1 Basic Concept of ElectricitysuarezОценок пока нет
- Seaward PR 15DДокумент2 страницыSeaward PR 15Dmuhdshafiq12Оценок пока нет
- VR6 Spec SheetДокумент4 страницыVR6 Spec Sheettuarek100% (1)
- Sewing Clutch Motor Pulley PDFДокумент15 страницSewing Clutch Motor Pulley PDFArja'un TeaОценок пока нет
- Lemon BatteryДокумент7 страницLemon BatteryVishal100% (8)
- SABIC Innovative Plastics Cycoloy C6200 PCABSДокумент3 страницыSABIC Innovative Plastics Cycoloy C6200 PCABSLex WangОценок пока нет
- Metric Conversion GuideДокумент36 страницMetric Conversion GuideAmmar A. Ali100% (2)
- Assessment Report On The Electrical Pump BreakdownsДокумент22 страницыAssessment Report On The Electrical Pump BreakdownsEdwin Cob GuriОценок пока нет