Вам также может понравиться
- American Credit Repair: Everything U Need to Know About Raising Your Credit ScoreОт EverandAmerican Credit Repair: Everything U Need to Know About Raising Your Credit ScoreРейтинг: 3 из 5 звезд3/5 (3)
- RAPID-P0027-0005-CON-JHA-3215-0005 - Rev. A JHA of Blasting and PaintingДокумент4 страницыRAPID-P0027-0005-CON-JHA-3215-0005 - Rev. A JHA of Blasting and Paintingshaiful annuarОценок пока нет
- CLG856H (GCIC 2 ZF Axle ZF210) OM 201910000-ENДокумент190 страницCLG856H (GCIC 2 ZF Axle ZF210) OM 201910000-ENManuel VenturaОценок пока нет
- Claim Preparation ManualДокумент15 страницClaim Preparation Manualasim46950% (2)
- Inspection and Test Plans (ITP) - MUM-05 Pump Installation ChecklistДокумент2 страницыInspection and Test Plans (ITP) - MUM-05 Pump Installation ChecklistAdades Safede EfdОценок пока нет
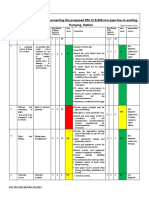
- Risk Assesment For Connecting The Existing Pipe To Pump StationДокумент4 страницыRisk Assesment For Connecting The Existing Pipe To Pump StationSasi Kumar100% (2)
- FRM-OHS-003 Management Review Meeting Minutes TemplateДокумент7 страницFRM-OHS-003 Management Review Meeting Minutes TemplateJoachimОценок пока нет
- fm2 0 PDFДокумент196 страницfm2 0 PDFJuan Palomo (Pajarito)Оценок пока нет
- First AidДокумент7 страницFirst AidRafal KrystosiakОценок пока нет
- ANSYS Mechanical APDL Fracture Analysis GuideДокумент178 страницANSYS Mechanical APDL Fracture Analysis GuideV Caf100% (1)
- JSA 03 Gate Entrance Traffic ProposalДокумент10 страницJSA 03 Gate Entrance Traffic Proposalrahul tkОценок пока нет
- INS 22 Reference Guide PDFДокумент57 страницINS 22 Reference Guide PDFRakesh MalhotaraОценок пока нет
- AccidentSickness E312 2022-10-9EDДокумент247 страницAccidentSickness E312 2022-10-9EDorlandoliuuОценок пока нет
- 02-011 Training & Development PolicyДокумент6 страниц02-011 Training & Development PolicyJoachimОценок пока нет
- 02-007 Machine and Equipment PolicyДокумент7 страниц02-007 Machine and Equipment PolicyJoachimОценок пока нет
- 02-009 Smoking PolicyДокумент6 страниц02-009 Smoking PolicyJoachimОценок пока нет
- 02-004 Electrical Installation PolicyДокумент7 страниц02-004 Electrical Installation PolicyJoachimОценок пока нет
- 02-010 Substance Abuse PolicyДокумент6 страниц02-010 Substance Abuse PolicyJoachimОценок пока нет
- 02-006 Injury On Duty (IOD) PolicyДокумент7 страниц02-006 Injury On Duty (IOD) PolicyJoachimОценок пока нет
- Lenskart Appliction FormДокумент6 страницLenskart Appliction FormEr Mayank UppalОценок пока нет
- 02-008 Personal Protective Equipment Issue PolicyДокумент6 страниц02-008 Personal Protective Equipment Issue PolicyJoachimОценок пока нет
- MOG-HSEQ-F-178 Major Accidents Notification FormДокумент2 страницыMOG-HSEQ-F-178 Major Accidents Notification FormSalim MuftahОценок пока нет
- 02-012 Working at Heights PolicyДокумент7 страниц02-012 Working at Heights PolicyJoachimОценок пока нет
- Power Distribution Works: Job Safety AnalysisДокумент30 страницPower Distribution Works: Job Safety AnalysisRekha LinusОценок пока нет
- 02-003 Environmental PolicyДокумент6 страниц02-003 Environmental PolicyJoachimОценок пока нет
- Health and Safety Inspection ReportДокумент6 страницHealth and Safety Inspection Reportapi-5487528040% (1)
- Ig2 Forms Electronic Submission v3Документ21 страницаIg2 Forms Electronic Submission v3Sajo JoseОценок пока нет
- 02-005 Hazardous Chemical Substance PolicyДокумент6 страниц02-005 Hazardous Chemical Substance PolicyJoachimОценок пока нет
- 02-001 Health, Safety and Environment PolicyДокумент7 страниц02-001 Health, Safety and Environment PolicyJoachimОценок пока нет
- 050 Musculoskeletal MFT FormДокумент2 страницы050 Musculoskeletal MFT FormScribd UserОценок пока нет
- Chapter - ThreeДокумент45 страницChapter - Threeadfsh-1Оценок пока нет
- Accident Record Sheet 1Документ2 страницыAccident Record Sheet 1ioanidteОценок пока нет
- 1 Page ContractДокумент2 страницы1 Page ContractAli M Al-anbaryОценок пока нет
- Mydoom Dom Anlysis Mydoom Virus - 568Документ44 страницыMydoom Dom Anlysis Mydoom Virus - 568Kheana Lany OperarioОценок пока нет
- Occupation Questionnaire PDFДокумент2 страницыOccupation Questionnaire PDFsuresh33% (3)
- S 000 1654 0130v - 0 - 0010 Emergency Response PlanДокумент45 страницS 000 1654 0130v - 0 - 0010 Emergency Response Planle huyОценок пока нет
- First Aid Incident ReportДокумент2 страницыFirst Aid Incident ReportBibin JohnОценок пока нет
- Corporation Bank Corp Personal: Application Cum AppraisalДокумент8 страницCorporation Bank Corp Personal: Application Cum Appraisalbalamurali sankaranarayananОценок пока нет
- COR-HSE-047 Accident Investigation ReportДокумент4 страницыCOR-HSE-047 Accident Investigation ReportMohamed Ali BoumarafОценок пока нет
- Industrial Waste Inspection Checklist Self Survey Ii - 124743Документ10 страницIndustrial Waste Inspection Checklist Self Survey Ii - 124743James DamwattОценок пока нет
- CGL Prop FormДокумент8 страницCGL Prop FormOmkar ChavanОценок пока нет
- 11.4 Form - COID - W.Cl.2 - Employers Report of An Accident PDFДокумент6 страниц11.4 Form - COID - W.Cl.2 - Employers Report of An Accident PDFJoachimОценок пока нет
- Risk Assessment Case Study - 1035Документ31 страницаRisk Assessment Case Study - 1035nmukherjee20Оценок пока нет
- EB 8310-6 EN: Translation of Original InstructionsДокумент72 страницыEB 8310-6 EN: Translation of Original InstructionsYandi HidayatОценок пока нет
- Occupation Questionnaire: Tataaia/Nb/Dm/46.1Документ2 страницыOccupation Questionnaire: Tataaia/Nb/Dm/46.1Xen Operation DPHОценок пока нет
- Indra: Incident Management PlanДокумент45 страницIndra: Incident Management Plantu VanОценок пока нет
- Registration Form: A. Personal InformationДокумент4 страницыRegistration Form: A. Personal InformationZulmy RhamadityaОценок пока нет
- Combined Liability Wording 121212Документ32 страницыCombined Liability Wording 121212rodd andertonОценок пока нет
- Property / Equipment Damage: General InformationДокумент2 страницыProperty / Equipment Damage: General InformationopytnymoryakОценок пока нет
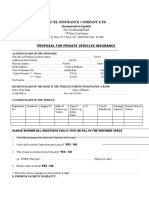
- FORM NO: U/014/130 Excel Insurance Company LTD: Proposal For Private Vehicles InsuranceДокумент2 страницыFORM NO: U/014/130 Excel Insurance Company LTD: Proposal For Private Vehicles Insuranceraymond ssegawaОценок пока нет
- 3rd Schedule Regulation 53 Written Declaration On Design and Construction of Industrial Effluent Treatment SystemДокумент2 страницы3rd Schedule Regulation 53 Written Declaration On Design and Construction of Industrial Effluent Treatment SystemLye lyeОценок пока нет
- 12 15 2015 Detective-Operations-ManualДокумент237 страниц12 15 2015 Detective-Operations-ManualMeljoriw 8496Оценок пока нет
- Technical Docu UM MSI-SR4B en 50124419Документ27 страницTechnical Docu UM MSI-SR4B en 50124419Amaresh DashОценок пока нет
- Incident Response DocumentationДокумент60 страницIncident Response DocumentationObad ZafarОценок пока нет
- Work Requition FromДокумент1 страницаWork Requition Fromremarkhb.maintenanceОценок пока нет
- English Application FormДокумент4 страницыEnglish Application FormFathu HasuОценок пока нет
- Approval and Registration of Third-Party Inspection Agencies For Lifting EquipmentДокумент47 страницApproval and Registration of Third-Party Inspection Agencies For Lifting Equipmentegy pureОценок пока нет
- Tbl-Retel-Aa-Sf-Pr-007 Confined Space ProcedureДокумент4 страницыTbl-Retel-Aa-Sf-Pr-007 Confined Space ProcedureMoaatazz NouisriОценок пока нет
- EOI Courtyard 62Документ2 страницыEOI Courtyard 62doc purushottamОценок пока нет
- Ref - DeterminationДокумент78 страницRef - Determinationpeoplessmile2000Оценок пока нет
- Windows Remote Desktop Heroes Villains - 7291Документ56 страницWindows Remote Desktop Heroes Villains - 7291Roohollah TavassoliОценок пока нет
- For Candidates With Ordinary Level QualificationДокумент3 страницыFor Candidates With Ordinary Level QualificationS HerathОценок пока нет
- SF-HSE-ForM-2 - 01-4b COID - W.cl.3 - Notice of Accident and Claim For CompensationДокумент2 страницыSF-HSE-ForM-2 - 01-4b COID - W.cl.3 - Notice of Accident and Claim For Compensationsjorgundson17Оценок пока нет
- WTO JudgementДокумент113 страницWTO JudgementMaha DevanОценок пока нет
- Motor Claim Form 2018111301Документ7 страницMotor Claim Form 2018111301Mike LorОценок пока нет
- Driver Questionnaire PDFДокумент2 страницыDriver Questionnaire PDFAman Trivedi0% (1)
- INLIAS - Integrated Non-Life Insurance Application Solution - User ManualДокумент30 страницINLIAS - Integrated Non-Life Insurance Application Solution - User Manualbirendra sonuОценок пока нет
- Manual Ifp Mn-00665Документ92 страницыManual Ifp Mn-00665Cristian SilvaОценок пока нет
- 1-Accident L Incident Investigation Report FormДокумент3 страницы1-Accident L Incident Investigation Report Formroland magoОценок пока нет
- Labour LawДокумент135 страницLabour LawSathish ChokkalingamОценок пока нет
- Civil Aviation QuestionnaireДокумент2 страницыCivil Aviation QuestionnairetatacrtОценок пока нет
- 118914-HDS-NT Mecha Ope Us-E04-201108Документ198 страниц118914-HDS-NT Mecha Ope Us-E04-201108jturnerОценок пока нет
- Postgrad App FormДокумент5 страницPostgrad App FormMohd ZubiОценок пока нет
- Britam Majnoon Guard Force Sops Aug 12Документ47 страницBritam Majnoon Guard Force Sops Aug 12IGP X-SQUAD FORCE HQTRSОценок пока нет
- Minnesota Handbook On Motor Vehicles Stops and Warrantless Searches 14 9Документ128 страницMinnesota Handbook On Motor Vehicles Stops and Warrantless Searches 14 9Wayne LundОценок пока нет
- Uz 2021 Postgraduate Application FormДокумент5 страницUz 2021 Postgraduate Application FormArnold TauroОценок пока нет
- Contractors Registration Board: Application Form For First Registration As Contractors By-Law 3 (1) (A)Документ17 страницContractors Registration Board: Application Form For First Registration As Contractors By-Law 3 (1) (A)Hubert MubofuОценок пока нет
- Stripping Machine S22: Operating InstructionsДокумент21 страницаStripping Machine S22: Operating InstructionsJavierОценок пока нет
- Raincoat & Gum Raincoat & Gumboot Boot: The Procurement of E-Tender For The Procurement ofДокумент19 страницRaincoat & Gum Raincoat & Gumboot Boot: The Procurement of E-Tender For The Procurement ofKarthick MahadevanОценок пока нет
- Practical Handbook for the Marketing of Foreign Investment Funds in Germany: A legal overviewОт EverandPractical Handbook for the Marketing of Foreign Investment Funds in Germany: A legal overviewОценок пока нет
- 200 PNT Final - March 16 2011Документ74 страницы200 PNT Final - March 16 2011JoachimОценок пока нет
- 03 Multi-Criteria Decision AnalysisДокумент4 страницы03 Multi-Criteria Decision AnalysisJoachimОценок пока нет
- Process Mapping Blank FormsДокумент3 страницыProcess Mapping Blank FormsJoachimОценок пока нет
- 02-002 Health, Safety and Environment Policy StatementДокумент2 страницы02-002 Health, Safety and Environment Policy StatementJoachimОценок пока нет
- Swot Form: Doc#: FRM-006 Rev: (2020-00) Project #: ( - ) Page 1 of 3Документ3 страницыSwot Form: Doc#: FRM-006 Rev: (2020-00) Project #: ( - ) Page 1 of 3JoachimОценок пока нет
- Assessor BookletДокумент4 страницыAssessor BookletJoachimОценок пока нет
- FRM-OHS-002 Management Review Agenda TemplateДокумент1 страницаFRM-OHS-002 Management Review Agenda TemplateJoachimОценок пока нет
- FRM-005 PESTLE TemplateДокумент4 страницыFRM-005 PESTLE TemplateJoachimОценок пока нет
- FRM OHS 001 Accident Incident Investigation TemplateДокумент3 страницыFRM OHS 001 Accident Incident Investigation TemplateJoachimОценок пока нет
- CHK-OHS-002 Contractors Health and Safety QuestionnaireДокумент3 страницыCHK-OHS-002 Contractors Health and Safety QuestionnaireJoachimОценок пока нет
- FRM-003 Role Profile FormДокумент1 страницаFRM-003 Role Profile FormJoachimОценок пока нет
- CHK-OHS-004 Safety Inspection - General Mechanical WorkshopДокумент2 страницыCHK-OHS-004 Safety Inspection - General Mechanical WorkshopJoachimОценок пока нет
- CHK-OHS-005 Safety Inspection - General OfficesДокумент2 страницыCHK-OHS-005 Safety Inspection - General OfficesJoachimОценок пока нет
- FRM-004 Training Evaluation FormДокумент1 страницаFRM-004 Training Evaluation FormJoachimОценок пока нет
- FRM-002 Document Change Request FormДокумент2 страницыFRM-002 Document Change Request FormJoachimОценок пока нет
- CHK-OHS-001 Contractor Supervision ChecklistДокумент1 страницаCHK-OHS-001 Contractor Supervision ChecklistJoachimОценок пока нет
- Fmcsa - Construction Contractors Safety InductionДокумент6 страницFmcsa - Construction Contractors Safety InductionJoachimОценок пока нет
- Accidents in Leisure Industry Jan. Through July 2023Документ30 страницAccidents in Leisure Industry Jan. Through July 2023Ly QuanОценок пока нет
- 10 - Neonaticide, Infanticide and Child HomicideДокумент45 страниц10 - Neonaticide, Infanticide and Child HomicideWala AbdeljawadОценок пока нет
- Translate - Indo Eng FINALДокумент6 страницTranslate - Indo Eng FINALJidanОценок пока нет
- ACL Tear InjuryДокумент5 страницACL Tear InjuryNicole VazОценок пока нет
- Maz - PRJ - Hse - PRC 11 - Manual Handling Procedure 001Документ5 страницMaz - PRJ - Hse - PRC 11 - Manual Handling Procedure 001ghazi kallelОценок пока нет
- KD Remasteredsheets Allupdated v4Документ17 страницKD Remasteredsheets Allupdated v4Apostolos KotselisОценок пока нет
- ASIA ISCOS IntlWorksheet 2019Документ2 страницыASIA ISCOS IntlWorksheet 2019Raquel GomesОценок пока нет
- Jsa-001 Manual Handling & Heavy LiftingДокумент2 страницыJsa-001 Manual Handling & Heavy LiftingDamien MonizeОценок пока нет
- BLS-First Aid (FTP-OJT) - 1Документ43 страницыBLS-First Aid (FTP-OJT) - 1TMRU TCPSОценок пока нет
- Lack of Time: Activity 3.2Документ2 страницыLack of Time: Activity 3.2Rodrigo De GuzmanОценок пока нет
- PCBL Form Medical Cert and WaiverДокумент1 страницаPCBL Form Medical Cert and WaiverEugene A. EstacioОценок пока нет
- Mechanical Engineering Level 2 NVQ by David Salmon and Penny PowdrillДокумент461 страницаMechanical Engineering Level 2 NVQ by David Salmon and Penny PowdrillfabianОценок пока нет
- WoundsДокумент2 страницыWoundsfive asiaticoОценок пока нет
- Death & Dismemberment: (By Josh "Bernie The Flumph" Burnett)Документ2 страницыDeath & Dismemberment: (By Josh "Bernie The Flumph" Burnett)Kevin CurtinОценок пока нет
- BCM 299 Assessment of An Injured PatientДокумент3 страницыBCM 299 Assessment of An Injured PatientTechnoveОценок пока нет
- Contractor Safety AuditДокумент1 страницаContractor Safety Auditmohamad ifthekharОценок пока нет
- Different Sports Injury and It'S Correct Wrapping and TappingДокумент27 страницDifferent Sports Injury and It'S Correct Wrapping and TappingSedney May JunioОценок пока нет
- Safety Toolbox Talk IdeasДокумент2 страницыSafety Toolbox Talk IdeasWendell Ryan OninezaОценок пока нет
- Safety Metrics Tools and Techniques For Measuring Performance Third Edition Ebook PDF VersionДокумент53 страницыSafety Metrics Tools and Techniques For Measuring Performance Third Edition Ebook PDF Versiondeborah.scott238100% (38)
- Forensic Science - 221117 - 211340Документ12 страницForensic Science - 221117 - 211340Lakhwinder BissarwalОценок пока нет
- Fireman's Rule and Its Extension To EMT'sДокумент7 страницFireman's Rule and Its Extension To EMT'sShahin DamouiОценок пока нет
- Determining Serious Injury and Fatality Exposure PotentialДокумент6 страницDetermining Serious Injury and Fatality Exposure PotentialISRAEL TOLANOОценок пока нет