Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Biostat and Research - PSS Sunder RaoДокумент279 страницBiostat and Research - PSS Sunder RaoPrincy Varghese67% (9)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Enzyme POGILДокумент6 страницEnzyme POGILnewhaventeacherОценок пока нет
- Globalresearch - Ca-Common Cruelty in Lockdown Time Allowing Hatred Fear and Paranoia To Cloud Our JudgmentДокумент6 страницGlobalresearch - Ca-Common Cruelty in Lockdown Time Allowing Hatred Fear and Paranoia To Cloud Our JudgmentJohn LewisОценок пока нет
- Oral Biologic Defenses in Tooth Demineralization and RemineralizationДокумент14 страницOral Biologic Defenses in Tooth Demineralization and RemineralizationWilson Fransiskus Chia GirsangОценок пока нет
- Risk For FallДокумент3 страницыRisk For FallLesValenzuela100% (1)
- Tipu Sultan History Painting and The Bat PDFДокумент47 страницTipu Sultan History Painting and The Bat PDFJohn LewisОценок пока нет
- The Dangerous Conspiracy Theories About The Zika VirusДокумент4 страницыThe Dangerous Conspiracy Theories About The Zika VirusJohn LewisОценок пока нет
- Globalresearch - Ca-Is The Lockdown The Greatest Policy Disaster in US HistoryДокумент6 страницGlobalresearch - Ca-Is The Lockdown The Greatest Policy Disaster in US HistoryJohn LewisОценок пока нет
- Globalresearch - Ca-The Farce and Diabolical Agenda of A Universal LockdownДокумент9 страницGlobalresearch - Ca-The Farce and Diabolical Agenda of A Universal LockdownJohn LewisОценок пока нет
- The Flu Vaccine A Shot in The DarkДокумент8 страницThe Flu Vaccine A Shot in The DarkJohn LewisОценок пока нет
- Globalresearch - Ca-Fear and Uncertainty The Modern-Day Cult of Corona Gotta To Have FaithДокумент10 страницGlobalresearch - Ca-Fear and Uncertainty The Modern-Day Cult of Corona Gotta To Have FaithJohn LewisОценок пока нет
- Globalresearch - ca-COVID Mask of The Beast and Deadly DistancingДокумент4 страницыGlobalresearch - ca-COVID Mask of The Beast and Deadly DistancingJohn LewisОценок пока нет
- Conspiracy-The Things People SayДокумент10 страницConspiracy-The Things People SayJohn LewisОценок пока нет
- Curvas NCДокумент3 страницыCurvas NCOscarPazRamirezОценок пока нет
- Biology Chapter 6 Solution Paper Grade 11 Advanced 2021-2022Документ8 страницBiology Chapter 6 Solution Paper Grade 11 Advanced 2021-2022mallmazОценок пока нет
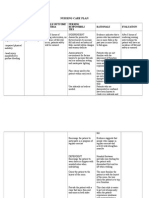
- Nursing Care Plan For Food PoisoningДокумент1 страницаNursing Care Plan For Food Poisoningscret_gurlz9220% (5)
- Cerebral Palsy Care Giving GuideДокумент511 страницCerebral Palsy Care Giving GuideJoel OntiverosОценок пока нет
- 19 - Symptoms, Signs and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00-R99) - 1Документ23 страницы19 - Symptoms, Signs and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00-R99) - 1Wardatul MukhlishohОценок пока нет
- 2nd Fattahi Morphophysiological and Phytochemical Responses To Cadmium and Lead Stress in Coriander (Coriandrum Sativum L.)Документ10 страниц2nd Fattahi Morphophysiological and Phytochemical Responses To Cadmium and Lead Stress in Coriander (Coriandrum Sativum L.)Mohammad Kazem souriОценок пока нет
- Mental Status ExaminationДокумент21 страницаMental Status ExaminationAthul RajОценок пока нет
- Breast Cancer Related Lymphedema2.pdfL P 4Документ12 страницBreast Cancer Related Lymphedema2.pdfL P 4LýОценок пока нет
- Module 1 Prenatal Development - PDF PDFДокумент11 страницModule 1 Prenatal Development - PDF PDFKevin PajarilloОценок пока нет
- Test Metodu EN1276 PDFДокумент13 страницTest Metodu EN1276 PDFhcsoyleyiciОценок пока нет
- Relief of Cancer Symptoms Through Art TherapyДокумент13 страницRelief of Cancer Symptoms Through Art TherapyCyanОценок пока нет
- 2011.7.endodontics and Periodontics Set 1Документ20 страниц2011.7.endodontics and Periodontics Set 1Loreto Mallabo MacadangdangОценок пока нет
- Histo LabДокумент6 страницHisto LabGAIL BATHANОценок пока нет
- Forrest GumpДокумент9 страницForrest GumpMeshack O SindaniОценок пока нет
- Mitanin Study FINALДокумент37 страницMitanin Study FINALAshok DadasОценок пока нет
- Hamilton Depression Rating Scale (HDRS) : VersionsДокумент3 страницыHamilton Depression Rating Scale (HDRS) : VersionsKristian Karl Bautista Kiw-isОценок пока нет
- Form LabДокумент1 страницаForm LabLab RS MMCОценок пока нет
- Bioquimica de La Isquemia y Reperfusion ArticuloДокумент35 страницBioquimica de La Isquemia y Reperfusion ArticulofelipeОценок пока нет
- RDPL Royal Diagnostics Pvt. Ltd.Документ6 страницRDPL Royal Diagnostics Pvt. Ltd.Royal Diagnostic Centre in Vaishali Nagar JaipurОценок пока нет
- Damps, Pamps, and Lamps in Immunity and Sterile InflammationДокумент26 страницDamps, Pamps, and Lamps in Immunity and Sterile InflammationCony G100% (1)
- Communicable Disease Nursing2Документ43 страницыCommunicable Disease Nursing2CAÑADA, JOHANNELYN M.Оценок пока нет
- Edukasi Penyuluhan AnemiaДокумент11 страницEdukasi Penyuluhan AnemiaRiza Nuraeni PutriОценок пока нет
- Cement Retained. Vs Screw Retained Implant (Ada GuideДокумент6 страницCement Retained. Vs Screw Retained Implant (Ada GuideAsma AbdullaОценок пока нет
- Support GroupsДокумент5 страницSupport Groupsapi-364431775Оценок пока нет
- Introduction To MycologyДокумент26 страницIntroduction To MycologyOsannah Irish InsongОценок пока нет
- NRT.011 Lui Freeze - Thaw ElutionДокумент4 страницыNRT.011 Lui Freeze - Thaw ElutionBrian LeungОценок пока нет