Вам также может понравиться
- CDC Covid-19 Report FormДокумент2 страницыCDC Covid-19 Report FormiggybauОценок пока нет
- Pui FormДокумент2 страницыPui FormBotez ElviraОценок пока нет
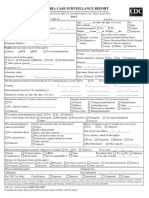
- Malaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Документ2 страницыMalaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Pramod gameОценок пока нет
- Cif NTДокумент2 страницыCif NTIvy marie BonОценок пока нет
- CIF-MR 2022 Ver1Документ2 страницыCIF-MR 2022 Ver1Ivy marie BonОценок пока нет
- Case Investigation Form - Measles-RubellaДокумент2 страницыCase Investigation Form - Measles-Rubellaclaverialc10Оценок пока нет
- HAEP CaseReport FormДокумент1 страницаHAEP CaseReport Formkaleem durraniОценок пока нет
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Документ3 страницыRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)テレビスマートОценок пока нет
- ReportForm TyphoidДокумент2 страницыReportForm TyphoidSundarajan ManiОценок пока нет
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDДокумент3 страницыViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaОценок пока нет
- Barangay Assisted Booking Form: CODE: D1AДокумент4 страницыBarangay Assisted Booking Form: CODE: D1AChristine May CagaraОценок пока нет
- CIF PertussisДокумент2 страницыCIF PertussisDan Joseph AguilarОценок пока нет
- Obstetrics History General DataДокумент7 страницObstetrics History General DataColeen NeyraОценок пока нет
- Multi Disciplinary Hosp Discharge PlanДокумент4 страницыMulti Disciplinary Hosp Discharge PlanDewi Angel BertОценок пока нет
- COVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersДокумент3 страницыCOVID-19 (Coronavirus) Exposure Questionnaire For Health Care WorkersDixit SushmithaОценок пока нет
- Veterans Memorial Medical Center: Medical Records Unit CR-1 Records of HospitalizationДокумент1 страницаVeterans Memorial Medical Center: Medical Records Unit CR-1 Records of Hospitalizationclaverialc10Оценок пока нет
- GordonsДокумент2 страницыGordonsAngelica OctotОценок пока нет
- Measles CIF 2014Документ2 страницыMeasles CIF 2014RionaMarieMagbutayОценок пока нет
- TX Section Short Label EN: Variable NameДокумент27 страницTX Section Short Label EN: Variable NamenasratullahОценок пока нет
- COVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsДокумент2 страницыCOVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsMovin PrabhakaranОценок пока нет
- CONSENT FORM - COVID-19 VaccineДокумент5 страницCONSENT FORM - COVID-19 Vaccinebersabeh abayОценок пока нет
- GM - FORMATO SINIESTROS - Medical ReportДокумент5 страницGM - FORMATO SINIESTROS - Medical ReportRicardo CadenaОценок пока нет
- ISARIC COVID-19 CRF V1.3 24feb2020Документ12 страницISARIC COVID-19 CRF V1.3 24feb2020ARINTA DWI KOMALAОценок пока нет
- PA 1 1 MergedДокумент9 страницPA 1 1 MergedMarc Mhel DalipeОценок пока нет
- Infectious Disease Medical Behavioral Screens AmendedДокумент6 страницInfectious Disease Medical Behavioral Screens AmendedHengkyОценок пока нет
- CRF HFMD AsmghДокумент2 страницыCRF HFMD AsmghRyeowook RyeОценок пока нет
- Case Report Form For HFMDДокумент2 страницыCase Report Form For HFMDMendez RhuОценок пока нет
- ANTENATAL Assessment FINALДокумент12 страницANTENATAL Assessment FINALM. jehovah Nissie YeshalomeОценок пока нет
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreДокумент2 страницыCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelОценок пока нет
- TX Section Short Label EN: Variable NameДокумент43 страницыTX Section Short Label EN: Variable NamelorenaОценок пока нет
- COVID-19 Patient Reporting Form: Reporter InformationДокумент2 страницыCOVID-19 Patient Reporting Form: Reporter InformationShinta Devianti100% (1)
- COVID-19 Vaccine Consent FormДокумент5 страницCOVID-19 Vaccine Consent FormSiamakОценок пока нет
- D ReportДокумент2 страницыD ReportHihiОценок пока нет
- HEALTH HISTORY GUIDE. ReviseДокумент2 страницыHEALTH HISTORY GUIDE. ReviseCathryn luv QuisidoОценок пока нет
- RCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Документ2 страницыRCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Mexico EnglishОценок пока нет
- New Axa FormДокумент2 страницыNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- Vaccine Consent For Meng 2021Документ2 страницыVaccine Consent For Meng 2021Eureka CassellОценок пока нет
- Nigeria ART Program Evaluation Data Extraction TooДокумент9 страницNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWОценок пока нет
- COVID-19 Test Request Form: Reporter InformationДокумент1 страницаCOVID-19 Test Request Form: Reporter InformationduckoduckОценок пока нет
- Measles Case FormДокумент3 страницыMeasles Case FormVlad BăhneanuОценок пока нет
- Patient QuestHHДокумент3 страницыPatient QuestHHAna RodriguezОценок пока нет
- Transfer Summary Form Hha To Hospital PDFДокумент2 страницыTransfer Summary Form Hha To Hospital PDFsafasayedОценок пока нет
- SLMC Consent For Treatment and Procedure During Covid19 PandemicДокумент2 страницыSLMC Consent For Treatment and Procedure During Covid19 PandemicCatie Tan ChingОценок пока нет
- Adverse Drug Reaction FormДокумент2 страницыAdverse Drug Reaction FormAre Pee Etc0% (1)
- Release MedicalInfo TOДокумент1 страницаRelease MedicalInfo TOChristinah Tamby LewanikaОценок пока нет
- Pidsr CifДокумент17 страницPidsr CifAbraham Asto100% (4)
- Portable Treatment RecordДокумент7 страницPortable Treatment RecordJОценок пока нет
- CASE-STUDY-psychiatric NursingДокумент16 страницCASE-STUDY-psychiatric NursingROSHANNEDANICA VERGARAОценок пока нет
- COVID Vaccination Packet SFOДокумент16 страницCOVID Vaccination Packet SFOferОценок пока нет
- Typhoid Fever Surveillance ReportДокумент2 страницыTyphoid Fever Surveillance ReportMarketing HydОценок пока нет
- Malaria Identification and Counseling FormДокумент1 страницаMalaria Identification and Counseling FormTewodros TafereОценок пока нет
- CDC Data Collection Long FormДокумент13 страницCDC Data Collection Long FormBanzai Health Private LimitedОценок пока нет
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityДокумент2 страницыHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaОценок пока нет
- 11 Trauma Emergency Form 19102023Документ2 страницы11 Trauma Emergency Form 19102023Marjorie BricenioОценок пока нет
- PUI Information CollectionДокумент3 страницыPUI Information CollectionAQUA VINES (official youtube channel)Оценок пока нет
- RabiesДокумент2 страницыRabiesninzah wanzahОценок пока нет
- Laboratory Sample Collection Form 3-22-2020Документ1 страницаLaboratory Sample Collection Form 3-22-2020Pradip Chandra SubediОценок пока нет
- Appendix A - FДокумент54 страницыAppendix A - Fbakson college gr. noidaОценок пока нет
- will it ever go away?: Practical Answers to Your Questions About COVID-19От Everandwill it ever go away?: Practical Answers to Your Questions About COVID-19Оценок пока нет
- New Zealand Homework SheetsДокумент6 страницNew Zealand Homework Sheetsdhbrvxsif100% (1)
- Neurology 1.03 Approach To Cerebral Function - Dr. MartinezДокумент7 страницNeurology 1.03 Approach To Cerebral Function - Dr. MartinezDeomicah SolanoОценок пока нет
- Perfection: Setting StandardsДокумент2 страницыPerfection: Setting StandardsGustavo MataОценок пока нет
- M.Pharm (PS) PCS PDFДокумент21 страницаM.Pharm (PS) PCS PDFDhruv BhandariОценок пока нет
- Republic of The Philippines: Scale Projects Are Defined As Those Construction Projects That Are Intended For PurelyДокумент12 страницRepublic of The Philippines: Scale Projects Are Defined As Those Construction Projects That Are Intended For PurelyBobby Olavides SebastianОценок пока нет
- Vital Signs PowerPointДокумент29 страницVital Signs PowerPointMeegs EstabilloОценок пока нет
- Interline 399+ds+eng PDFДокумент4 страницыInterline 399+ds+eng PDFMohamed NouzerОценок пока нет
- (Human) : Joyce Travelbee To Human RelationshipДокумент3 страницы(Human) : Joyce Travelbee To Human RelationshipJhanice Pejo PolicarpioОценок пока нет
- 2022 Annual ReportДокумент76 страниц2022 Annual ReportLive 5 NewsОценок пока нет
- Detail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshДокумент156 страницDetail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshPriety Verma91% (11)
- THBHDK 15Документ1 страницаTHBHDK 15RGNitinDevaОценок пока нет
- Health EducationДокумент7 страницHealth Educationmylene lingonОценок пока нет
- Managerial Skill Development Unit-3Документ44 страницыManagerial Skill Development Unit-3Arif QuadriОценок пока нет
- What Is Mental Health Illness ContinuumДокумент2 страницыWhat Is Mental Health Illness ContinuumAileen A. MonaresОценок пока нет
- Leica Rm2125rts Ifu 2v8l enДокумент68 страницLeica Rm2125rts Ifu 2v8l enNguyen Trung HuyОценок пока нет
- Amjad Iqbal: ObjectiveДокумент17 страницAmjad Iqbal: ObjectiveKhalid HussainОценок пока нет
- Random Blood Sugar Test AssignmentДокумент1 страницаRandom Blood Sugar Test AssignmentmadamcloudnineОценок пока нет
- BBH 411w Final Project Narrative Literature ReviewДокумент27 страницBBH 411w Final Project Narrative Literature Reviewapi-582674998Оценок пока нет
- I. Choose The Most Correct Answer:: Page 1 To 9Документ9 страницI. Choose The Most Correct Answer:: Page 1 To 9Hasan A AsFourОценок пока нет
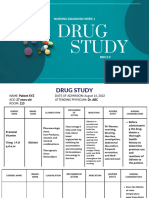
- Study: Nursing Diagnosis Week 1Документ9 страницStudy: Nursing Diagnosis Week 122 - Fernandez, Lyza Mae D.Оценок пока нет
- Red Team ChecklistДокумент2 страницыRed Team ChecklistChristine Joy BautistaОценок пока нет
- Rama College of Nursing: Health Education OnДокумент24 страницыRama College of Nursing: Health Education OnBrijesh Yadav100% (1)
- HD 60364-7-710Документ46 страницHD 60364-7-710LUis Faria100% (2)
- Garcia v. Salvador G.R. NO. 168512, March 20, 2007Документ9 страницGarcia v. Salvador G.R. NO. 168512, March 20, 2007ChatОценок пока нет
- Nursing Philosohy ApaДокумент4 страницыNursing Philosohy Apaapi-520823631Оценок пока нет
- CA HDKN Wacker YA47895 & YA47897 PDFДокумент4 страницыCA HDKN Wacker YA47895 & YA47897 PDFSatak ArHundaОценок пока нет
- The 12-Lead ElectrocardiogramДокумент16 страницThe 12-Lead ElectrocardiogramGrace Rivera GuarinОценок пока нет
- Sri Mulyani PDFДокумент7 страницSri Mulyani PDFHasna RofifahОценок пока нет
- DEvinДокумент7 страницDEvinTuriyo AnthonyОценок пока нет
- Organ Transplantation Is Considered A Medical Miracle of The 20th CenturyДокумент142 страницыOrgan Transplantation Is Considered A Medical Miracle of The 20th CenturyVaibhav SharmaОценок пока нет