Вам также может понравиться
- Quezon City Department of The Building OfficialДокумент2 страницыQuezon City Department of The Building OfficialBrightNotes86% (7)
- BRD TemplateДокумент4 страницыBRD TemplateTrang Nguyen0% (1)
- FT Goblin Full SizeДокумент7 страницFT Goblin Full SizeDeakon Frost100% (1)
- 2.8 V6 5V (Aha & Atq)Документ200 страниц2.8 V6 5V (Aha & Atq)Vladimir Socin ShakhbazyanОценок пока нет
- Hospital Future Augmented - Reality - in - SurgeryДокумент10 страницHospital Future Augmented - Reality - in - Surgeryroupen sulahianОценок пока нет
- Longo Et Al 2021 Augmented Reality, Virtual ReaДокумент13 страницLongo Et Al 2021 Augmented Reality, Virtual ReaLeandro Magno Correa da SilvaОценок пока нет
- New Technology in Medical ImagingДокумент5 страницNew Technology in Medical ImagingAli BirОценок пока нет
- A Literature Review On Techniques For Detection of Lung DiseasesДокумент8 страницA Literature Review On Techniques For Detection of Lung DiseasesIJRASETPublicationsОценок пока нет
- Automatic Detection of Tuberculosis Related Abnormalities in Chest X-Ray Images Using Hierarchical FДокумент17 страницAutomatic Detection of Tuberculosis Related Abnormalities in Chest X-Ray Images Using Hierarchical FReadoy RahmanОценок пока нет
- The Role of Virtual and Augmented Reality in Ortho - 2020 - Computer Methods andДокумент11 страницThe Role of Virtual and Augmented Reality in Ortho - 2020 - Computer Methods andAndres ChiribogaОценок пока нет
- 11.deep Learning Applications in Medical Image Analysis-Brain TumorДокумент4 страницы11.deep Learning Applications in Medical Image Analysis-Brain TumorVenky Naidu BalineniОценок пока нет
- Bjs 9711Документ15 страницBjs 9711Bintang MuslimahОценок пока нет
- ìºÏÏÖÊ ÊõÔÚÒ Ñ ÊÖÊõ¿ÉÊÓ ÖÐ ÄÓ ÓÃÑÐ ¿Документ7 страницìºÏÏÖÊ ÊõÔÚÒ Ñ ÊÖÊõ¿ÉÊÓ ÖÐ ÄÓ ÓÃÑÐ ¿Anonymous HUY0yRexYfОценок пока нет
- Fully Automated 3D Colon Segmentation and Volume Rendering in Virtual RealityДокумент9 страницFully Automated 3D Colon Segmentation and Volume Rendering in Virtual RealityJamil Al-idrusОценок пока нет
- Multimodal Medical Image Fusion Using Stacked Auto Encoder in NSCT DomainДокумент18 страницMultimodal Medical Image Fusion Using Stacked Auto Encoder in NSCT DomainShrida Prathamesh KalamkarОценок пока нет
- A Systematic Review On Artificial Intelligence ForДокумент20 страницA Systematic Review On Artificial Intelligence ForblueyoonvОценок пока нет
- Radiomics in Medical Imaging - "How-To" Guide and Critical ReflectionДокумент16 страницRadiomics in Medical Imaging - "How-To" Guide and Critical ReflectionAxcОценок пока нет
- Augmented Reality As A Telemedicine Platform For RДокумент21 страницаAugmented Reality As A Telemedicine Platform For Rjeromesweety3Оценок пока нет
- Future Trends and Technologies in Interventional Radiology: What To ExpectДокумент6 страницFuture Trends and Technologies in Interventional Radiology: What To Expectmalavikasureshkumar7Оценок пока нет
- Augmented-Reality-Based-Visual-Haptic-Modeling-For 2021 Virtual-Reality - inДокумент13 страницAugmented-Reality-Based-Visual-Haptic-Modeling-For 2021 Virtual-Reality - inapi-688059491Оценок пока нет
- Implementation of CT Image Segmentation Based On AДокумент11 страницImplementation of CT Image Segmentation Based On AZAHRA FASKAОценок пока нет
- Mixed Reality 2021Документ16 страницMixed Reality 2021MadhanDhonianОценок пока нет
- CH 3Документ21 страницаCH 3Mohamed AhmedОценок пока нет
- Predictive Analytics Healthcare SurgeryДокумент3 страницыPredictive Analytics Healthcare SurgerylauОценок пока нет
- Artículo CirugíaДокумент11 страницArtículo CirugíaVictor ValdiviaОценок пока нет
- Accuracy of Digital and Analogue Cephalometric Measurements Assessed With The Sandwich TechniqueДокумент7 страницAccuracy of Digital and Analogue Cephalometric Measurements Assessed With The Sandwich TechniqueNurulArifahОценок пока нет
- Automated Chest Screening Based On A Hybrid Model of Transfer Learning and Convolutional Sparse Denoising AutoencoderДокумент19 страницAutomated Chest Screening Based On A Hybrid Model of Transfer Learning and Convolutional Sparse Denoising AutoencoderAlejandro De Jesus Romo RosalesОценок пока нет
- Artificial Intelligence in Diagnostic Pathology: Review Open AccessДокумент12 страницArtificial Intelligence in Diagnostic Pathology: Review Open Accessgupta.mridula2014Оценок пока нет
- Jud2020 Article ApplicabilityOfAugmentedRealitДокумент13 страницJud2020 Article ApplicabilityOfAugmentedRealitmohadeseОценок пока нет
- Virtual Surgery 07012013125131 Virtual SurgeryДокумент20 страницVirtual Surgery 07012013125131 Virtual Surgeryjosemonj77Оценок пока нет
- Computer Methods and Programs in BiomedicineДокумент15 страницComputer Methods and Programs in BiomedicineDr Mohammed KamalОценок пока нет
- A Comparative Study of Tuberculosis DetectionДокумент5 страницA Comparative Study of Tuberculosis DetectionMehera Binte MizanОценок пока нет
- Augmented Reality Visualization For Image Guided SДокумент10 страницAugmented Reality Visualization For Image Guided SPaulo Ferreira OrtodontiaОценок пока нет
- Survey of Explainable Artificial Intelligence Techniques For Biomedical Imaging With Deep Neural NetworksДокумент29 страницSurvey of Explainable Artificial Intelligence Techniques For Biomedical Imaging With Deep Neural Networkslenka14126Оценок пока нет
- 1 s2.0 S2666521221000090 MainДокумент18 страниц1 s2.0 S2666521221000090 MainMEHDI JAHANIRADОценок пока нет
- ResNet-50 Vs VGG-19 Vs Training From Scratch A Comparative Analysis of The Segmentation and Classification of Pneumonia FromДокумент10 страницResNet-50 Vs VGG-19 Vs Training From Scratch A Comparative Analysis of The Segmentation and Classification of Pneumonia FromCarlos Cézar ConradОценок пока нет
- Seminar ReportДокумент30 страницSeminar ReportKhadeeja AshnaОценок пока нет
- Assessment of The Accuracy of Imaging Software For 3D Rendering of The Upper Airway, Usable in Orthodontic and Craniofacial Clinical SettingsДокумент14 страницAssessment of The Accuracy of Imaging Software For 3D Rendering of The Upper Airway, Usable in Orthodontic and Craniofacial Clinical SettingsPhachara SiripraphonrojОценок пока нет
- Advances in Ultrasound Imaging Techniques and Applications A Comprehensive ReviewДокумент3 страницыAdvances in Ultrasound Imaging Techniques and Applications A Comprehensive ReviewTrésor NaraОценок пока нет
- A Rapid Calibration Method For Registration and 3D Tracking of Ultrasound Images Using Spatial LocalizerДокумент12 страницA Rapid Calibration Method For Registration and 3D Tracking of Ultrasound Images Using Spatial Localizerعامر العليОценок пока нет
- A Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT ScannersДокумент11 страницA Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT Scannershectorkevin2008Оценок пока нет
- State-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant PlacementДокумент7 страницState-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant Placementanimeilove3Оценок пока нет
- Augmented Reality in Medicine SCOPEДокумент3 страницыAugmented Reality in Medicine SCOPESK sriraamОценок пока нет
- Savadjiev2018 Article DemystificationOfAI-drivenMediДокумент9 страницSavadjiev2018 Article DemystificationOfAI-drivenMediAnna LeeОценок пока нет
- Seminar Report On Virtual SurgeryДокумент17 страницSeminar Report On Virtual SurgeryAfrah RamsheedОценок пока нет
- Lung Cancer Detection Using Fusion, CNN and YOLO in MATLABДокумент10 страницLung Cancer Detection Using Fusion, CNN and YOLO in MATLABIJRASETPublicationsОценок пока нет
- An Overview of Artificial Intelligence in Medical Physics and Radiation OncologyДокумент11 страницAn Overview of Artificial Intelligence in Medical Physics and Radiation Oncologyxiwevi4103Оценок пока нет
- Computer Aided DiagnosisДокумент20 страницComputer Aided Diagnosisnigel989Оценок пока нет
- Volumetric 3D Display For Radiation Therapy PlanningДокумент28 страницVolumetric 3D Display For Radiation Therapy PlanningNewberryОценок пока нет
- Ultrasound Machine Research PaperДокумент5 страницUltrasound Machine Research Paperpukytij0wyg3100% (1)
- 2023-智能图像配准-attention guided refine and deformationДокумент13 страниц2023-智能图像配准-attention guided refine and deformationbo zhaoОценок пока нет
- CAS Craniomaxillofacial Surgery PlanningДокумент18 страницCAS Craniomaxillofacial Surgery Planninghasan nazzalОценок пока нет
- Augmented Reality: Augmented Reality (AR) Is An Interactive Experience of A Real-World EnvironmentДокумент4 страницыAugmented Reality: Augmented Reality (AR) Is An Interactive Experience of A Real-World EnvironmentamleyyОценок пока нет
- Research Article Enhance-Net: An Approach To Boost The Performance of Deep Learning Model Based On Real-Time Medical ImagesДокумент15 страницResearch Article Enhance-Net: An Approach To Boost The Performance of Deep Learning Model Based On Real-Time Medical ImagesFilip PajićОценок пока нет
- A Technological Breakthrough: Empowering Breast Cancer Imaging Through Augmented Reality Visualization On Android Based PlatformsДокумент5 страницA Technological Breakthrough: Empowering Breast Cancer Imaging Through Augmented Reality Visualization On Android Based PlatformsInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- A Novel Deep Learning Framework For Lung Nodule Detection in 3d CT ImagesДокумент17 страницA Novel Deep Learning Framework For Lung Nodule Detection in 3d CT Imagesdreadrebirth2342Оценок пока нет
- DMF 41 011 PDFДокумент7 страницDMF 41 011 PDFDenis KimОценок пока нет
- PHD Thesis On Medical Image FusionДокумент6 страницPHD Thesis On Medical Image Fusionmeghanhowardmanchester100% (2)
- Technical Seminar PPTДокумент15 страницTechnical Seminar PPTshashidharsykОценок пока нет
- Artificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglДокумент2 страницыArtificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglMomoh GaiusОценок пока нет
- Lung Cancer Detection Using CT Scan Images: SciencedirectДокумент8 страницLung Cancer Detection Using CT Scan Images: SciencedirectPavan KumarОценок пока нет
- Sensors 22 01478 v2Документ17 страницSensors 22 01478 v2Simi Florin CiraОценок пока нет
- Sensors 21 02927Документ16 страницSensors 21 02927Ashish Presanna ChandranОценок пока нет
- Hybrid In-Situ Visualization Method For Improving Multi-Sensory Depth Perception inДокумент10 страницHybrid In-Situ Visualization Method For Improving Multi-Sensory Depth Perception inSK sriraamОценок пока нет
- A Survey of Augmented Reality PDFДокумент31 страницаA Survey of Augmented Reality PDFSK sriraamОценок пока нет
- Folia Medica) Striving For Better Medical Education - The Simulation ApproachДокумент9 страницFolia Medica) Striving For Better Medical Education - The Simulation ApproachSK sriraamОценок пока нет
- Augmented Reality in Medicine SCOPEДокумент3 страницыAugmented Reality in Medicine SCOPESK sriraamОценок пока нет
- Bharat Sanchar Nigam Limited: Receipt DetailsДокумент1 страницаBharat Sanchar Nigam Limited: Receipt DetailsSK sriraamОценок пока нет
- Augmented Reality in Medical Education and TrainingДокумент7 страницAugmented Reality in Medical Education and Trainingfuki nanginamoОценок пока нет
- Augmented Reality in Medical Education and TrainingДокумент7 страницAugmented Reality in Medical Education and Trainingfuki nanginamoОценок пока нет
- Marker-Less Real Time Intra-Operative Camera and HДокумент7 страницMarker-Less Real Time Intra-Operative Camera and HSK sriraamОценок пока нет
- Advanced Medical Displays A Literature Review of PDFДокумент17 страницAdvanced Medical Displays A Literature Review of PDFSK sriraamОценок пока нет
- 237 Nature Materials 10 532-538 2011Документ7 страниц237 Nature Materials 10 532-538 2011SK sriraamОценок пока нет
- Augmented Reality in Medical Education A Systematic Review PDFДокумент16 страницAugmented Reality in Medical Education A Systematic Review PDFSK sriraamОценок пока нет
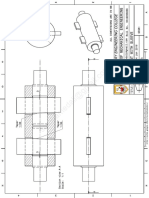
- 012 CotterWithSleeve Class Work 21stjan2016Документ5 страниц012 CotterWithSleeve Class Work 21stjan2016SK sriraamОценок пока нет
- Screw JackДокумент7 страницScrew JackSK sriraamОценок пока нет
- Preface To The Third EditionДокумент3 страницыPreface To The Third EditionSK sriraamОценок пока нет
- 012 CotterWithSleeve Class Work 21stjan2016Документ5 страниц012 CotterWithSleeve Class Work 21stjan2016SK sriraamОценок пока нет
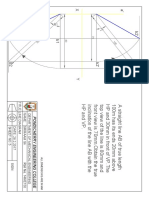
- Line DiagramДокумент1 страницаLine DiagramSK sriraamОценок пока нет
- Non VerbalДокумент28 страницNon VerbalSK sriraamОценок пока нет
- Thermal NotesДокумент112 страницThermal NotesSK sriraamОценок пока нет
- StandardsДокумент3 страницыStandardshappystamps100% (1)
- Cercado VsДокумент1 страницаCercado VsAnn MarieОценок пока нет
- Sapkale Sandspit 2020Документ5 страницSapkale Sandspit 2020jbs_geoОценок пока нет
- Ju Complete Face Recovery GAN Unsupervised Joint Face Rotation and De-Occlusion WACV 2022 PaperДокумент11 страницJu Complete Face Recovery GAN Unsupervised Joint Face Rotation and De-Occlusion WACV 2022 PaperBiponjot KaurОценок пока нет
- 7th Kannada Science 01Документ160 страниц7th Kannada Science 01Edit O Pics StatusОценок пока нет
- Module 5Документ10 страницModule 5kero keropiОценок пока нет
- Enerflex 381338Документ2 страницыEnerflex 381338midoel.ziatyОценок пока нет
- Entrepreneurship WholeДокумент20 страницEntrepreneurship WholeKrizztian SiuaganОценок пока нет
- Yi-Lai Berhad - COMPANY PROFILE - ProjectДокумент4 страницыYi-Lai Berhad - COMPANY PROFILE - ProjectTerry ChongОценок пока нет
- Account STMT XX0226 19122023Документ13 страницAccount STMT XX0226 19122023rdineshyОценок пока нет
- Introduction To Succession-1Документ8 страницIntroduction To Succession-1amun dinОценок пока нет
- 13-07-01 Declaration in Support of Skyhook Motion To CompelДокумент217 страниц13-07-01 Declaration in Support of Skyhook Motion To CompelFlorian MuellerОценок пока нет
- Mba Assignment SampleДокумент5 страницMba Assignment Sampleabdallah abdОценок пока нет
- Project The Ant Ranch Ponzi Scheme JDДокумент7 страницProject The Ant Ranch Ponzi Scheme JDmorraz360Оценок пока нет
- Salary Slip Oct PacificДокумент1 страницаSalary Slip Oct PacificBHARAT SHARMAОценок пока нет
- Royalty-Free License AgreementДокумент4 страницыRoyalty-Free License AgreementListia TriasОценок пока нет
- Top 35 Brokerage Firms in PakistanДокумент11 страницTop 35 Brokerage Firms in PakistannasiralisauОценок пока нет
- NAC Case Study AnalysisДокумент25 страницNAC Case Study AnalysisSushma chhetriОценок пока нет
- 3 Course Contents IIIBДокумент5 страниц3 Course Contents IIIBshahabОценок пока нет
- Novirost Sample TeaserДокумент2 страницыNovirost Sample TeaserVlatko KotevskiОценок пока нет
- Top Brand Story Bar Supervisor Jobs Chennai Apply Now Latest Fresher Experienced Bar Supervisor Jobs in Various Location July 18 2021Документ1 страницаTop Brand Story Bar Supervisor Jobs Chennai Apply Now Latest Fresher Experienced Bar Supervisor Jobs in Various Location July 18 2021Surya JamesОценок пока нет
- Part I-Final Report On Soil InvestigationДокумент16 страницPart I-Final Report On Soil InvestigationmangjuhaiОценок пока нет
- Aptio ™ Text Setup Environment (TSE) User ManualДокумент42 страницыAptio ™ Text Setup Environment (TSE) User Manualdhirender karkiОценок пока нет
- SD Electrolux LT 4 Partisi 21082023Документ3 страницыSD Electrolux LT 4 Partisi 21082023hanifahОценок пока нет
- Learning HotMetal Pro 6 - 132Документ332 страницыLearning HotMetal Pro 6 - 132Viên Tâm LangОценок пока нет
- Discursive Closure and Discursive Openings in SustainabilityДокумент10 страницDiscursive Closure and Discursive Openings in SustainabilityRenn MОценок пока нет