Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- New Anti-Corrosion Methods For Marine Steel StructuresДокумент10 страницNew Anti-Corrosion Methods For Marine Steel Structuresrigonz2Оценок пока нет
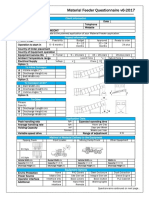
- Material Feeder Questionnaire v6 2017Документ3 страницыMaterial Feeder Questionnaire v6 2017rigonz2Оценок пока нет
- Travel and Shipping Before The RailroadsДокумент13 страницTravel and Shipping Before The Railroadsrigonz2Оценок пока нет
- US Systems Cyclone Separator PDFДокумент1 страницаUS Systems Cyclone Separator PDFrigonz2Оценок пока нет
- Arctic Marine Operations Report PDFДокумент463 страницыArctic Marine Operations Report PDFrigonz2Оценок пока нет
- Ceramic Capacitors, Murata PDFДокумент70 страницCeramic Capacitors, Murata PDFrigonz2Оценок пока нет
- Comparison of APEC Wind Loading and Chinese National CodeДокумент14 страницComparison of APEC Wind Loading and Chinese National Coderigonz2Оценок пока нет
- Dry Bulk Shipping INvestment, 2016Документ8 страницDry Bulk Shipping INvestment, 2016rigonz2Оценок пока нет
- Deterioration and Restoration of Concrete Jetties PDFДокумент10 страницDeterioration and Restoration of Concrete Jetties PDFrigonz2Оценок пока нет
- Bulk Transport Factsheet 2013Документ3 страницыBulk Transport Factsheet 2013rigonz2Оценок пока нет
- Is 8730 97 Bulk MaterialsДокумент25 страницIs 8730 97 Bulk Materialsrigonz2100% (1)
- European Code For Inland WaterwaysДокумент5 страницEuropean Code For Inland Waterwaysrigonz2Оценок пока нет
- Silo Technology, Cones and CodesДокумент8 страницSilo Technology, Cones and Codesrigonz2Оценок пока нет
- Anchor ManualДокумент187 страницAnchor ManualAde Aris Satria100% (5)
- High Volume Flyash Concrete PDFДокумент18 страницHigh Volume Flyash Concrete PDFrigonz2Оценок пока нет
- Embankment Over Soft ClayДокумент14 страницEmbankment Over Soft Clayrigonz2Оценок пока нет
- LV Motors Catalogue, TecoДокумент128 страницLV Motors Catalogue, Tecorigonz2Оценок пока нет
- Structural Optimization of Turbo Generator FoundationДокумент10 страницStructural Optimization of Turbo Generator Foundationrigonz2Оценок пока нет
- Hyperconnected Economy 02, EIUДокумент26 страницHyperconnected Economy 02, EIUrigonz2Оценок пока нет
- Manual For Evaluation of Industrial Projects, UNIDOДокумент151 страницаManual For Evaluation of Industrial Projects, UNIDOrigonz2Оценок пока нет
- CIP23 Discoloration PDFДокумент0 страницCIP23 Discoloration PDFrigonz2Оценок пока нет
- Development Economics Through The Decades, WBДокумент206 страницDevelopment Economics Through The Decades, WBrigonz2100% (3)
- Codal Provisions For Design of Machine Foundations - A ReviewДокумент6 страницCodal Provisions For Design of Machine Foundations - A Reviewrigonz2Оценок пока нет
- PB Network 76 Pathways To Innovation PDFДокумент84 страницыPB Network 76 Pathways To Innovation PDFrigonz2Оценок пока нет
- FM 55-21 Railway Operating and Safety RulesДокумент254 страницыFM 55-21 Railway Operating and Safety Rulesrigonz2Оценок пока нет
- Floating Point ComputationДокумент123 страницыFloating Point Computationrigonz2Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Mis 121620003Документ39 страницMis 121620003Gaurav PawarОценок пока нет
- Performance Level Basic: English Language Arts (ELA) Performance Level Definitions ACTAAP Grade 5 Benchmark ExaminationsДокумент3 страницыPerformance Level Basic: English Language Arts (ELA) Performance Level Definitions ACTAAP Grade 5 Benchmark ExaminationsKinray BadeОценок пока нет
- Measuring and Managing Brand LoyaltyДокумент18 страницMeasuring and Managing Brand Loyaltyshyl00ksОценок пока нет
- Name: - Track: - ScoreДокумент2 страницыName: - Track: - ScoreDA FTОценок пока нет
- Employee Behavior in Organizations: On The Current State of ResearchДокумент24 страницыEmployee Behavior in Organizations: On The Current State of ResearchCaladhielОценок пока нет
- Doe STD 1197 2011Документ123 страницыDoe STD 1197 2011Marco RangelОценок пока нет
- Topic 1 Management Commitment6 PDFДокумент50 страницTopic 1 Management Commitment6 PDFDiyana OsmanОценок пока нет
- Management Concepts and Practices BBAC 0001Документ21 страницаManagement Concepts and Practices BBAC 0001Ashutosh SinghОценок пока нет
- The Master Key System by Charles F. HaanelДокумент214 страницThe Master Key System by Charles F. HaanelFrancisco Sousa100% (1)
- PMP Lite Mock Exam 2 QuestionsДокумент16 страницPMP Lite Mock Exam 2 QuestionsJobin John100% (1)
- Machine and Ecology: AngelakiДокумент14 страницMachine and Ecology: Angelakifilter547Оценок пока нет
- SFTY100 QuestionsДокумент3 страницыSFTY100 QuestionsKlydeJoseОценок пока нет
- Identifying and Solving The Five Types of Process ProblemsДокумент185 страницIdentifying and Solving The Five Types of Process ProblemsLupo Alberto100% (1)
- FFAPUSH Skills and Writing Guidelines PDFДокумент23 страницыFFAPUSH Skills and Writing Guidelines PDFAnish ChitnisОценок пока нет
- WSHC Case Studies Chemical IndustryДокумент76 страницWSHC Case Studies Chemical IndustrySanthosh Kumar50% (2)
- SHOTWELL, James. The Interpretation of HistoryДокумент19 страницSHOTWELL, James. The Interpretation of HistoryFelipe Cabral100% (1)
- The Philosophy of The Social Sciences by Alan Ryan-204-225Документ22 страницыThe Philosophy of The Social Sciences by Alan Ryan-204-225akshita aggarwalОценок пока нет
- Chapter 7 (Part II)Документ27 страницChapter 7 (Part II)AmolShahОценок пока нет
- Mancur Olson The Rise and Decline of NationsДокумент289 страницMancur Olson The Rise and Decline of NationsTural Hazrat100% (1)
- Construction LawДокумент45 страницConstruction LawChandima SrimaliОценок пока нет
- Analyzing Activity and Injury: Lessons Learned From The Acute:Chronic Workload RatioДокумент12 страницAnalyzing Activity and Injury: Lessons Learned From The Acute:Chronic Workload RatioLukas ArenasОценок пока нет
- Causes of Salvadoran Migration To The United StatesДокумент13 страницCauses of Salvadoran Migration To The United Statesasek1Оценок пока нет
- Contemporary WarfareДокумент16 страницContemporary WarfareASUPREMEAОценок пока нет
- Special RelativityДокумент236 страницSpecial RelativityAndrei Avadani100% (3)
- MMDS PDFДокумент1 241 страницаMMDS PDFyusnitaОценок пока нет
- Hastrup, Kirsten - Getting It RightДокумент19 страницHastrup, Kirsten - Getting It RightMark Friis McHauОценок пока нет
- Translating The Term Paticcasamuppada Into EnglishДокумент8 страницTranslating The Term Paticcasamuppada Into EnglishDhammarathana IlukewelaОценок пока нет
- Process Theory The Principles of Operations Manage... - (1 The Discipline of Operations Management) PDFДокумент30 страницProcess Theory The Principles of Operations Manage... - (1 The Discipline of Operations Management) PDFSunny SouravОценок пока нет
- The Athenian EmpireДокумент107 страницThe Athenian EmpireAngelo_ColonnaОценок пока нет
- ACCT2522 Final NotesДокумент38 страницACCT2522 Final Noteskittyangel_01100% (1)