Вам также может понравиться
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementОт EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouОценок пока нет
- Effects of Short-Course Oral Corticosteroid Therapy in Early Dengue Infection in Vietnamese Patients: A Randomized, Placebo-Controlled TrialДокумент10 страницEffects of Short-Course Oral Corticosteroid Therapy in Early Dengue Infection in Vietnamese Patients: A Randomized, Placebo-Controlled TrialJihadatul KholilahОценок пока нет
- Prediction of Dengue Disease Severity Among Pediatric Thai Patients Using Early Clinical Laboratory IndicatorsДокумент7 страницPrediction of Dengue Disease Severity Among Pediatric Thai Patients Using Early Clinical Laboratory Indicatorsnita_hasnitaОценок пока нет
- Nifurtimox 1Документ7 страницNifurtimox 1AYUSH DUBEYОценок пока нет
- Neutropenic Colitis in Children 2011Документ4 страницыNeutropenic Colitis in Children 2011IRINA SULEY TIRADO PEREZОценок пока нет
- Dengue Hemorrhagic Fever: The Sensitivity and Specificity of The World Health Organization Definition For Identification of Severe Cases of Dengue in Thailand, 1994-2005Документ10 страницDengue Hemorrhagic Fever: The Sensitivity and Specificity of The World Health Organization Definition For Identification of Severe Cases of Dengue in Thailand, 1994-2005Dessy AmaranthaОценок пока нет
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsДокумент9 страницResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998Оценок пока нет
- Journal PNTD 0001244Документ10 страницJournal PNTD 0001244Zulia Ahmad BurhaniОценок пока нет
- BJC 2017154Документ8 страницBJC 2017154Altair CamargoОценок пока нет
- Risk Factors For Mortality in Patients With DengueДокумент13 страницRisk Factors For Mortality in Patients With DengueTaufiqurrokhman RofiiОценок пока нет
- Journal of Pediatric HematologyДокумент10 страницJournal of Pediatric HematologyasepОценок пока нет
- Risk Factors For Herpes Zoster in Patients With Chronic Kidney Disease: A Case-Control StudyДокумент7 страницRisk Factors For Herpes Zoster in Patients With Chronic Kidney Disease: A Case-Control StudyPushpendra Singh ChouhanОценок пока нет
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorДокумент6 страницIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasОценок пока нет
- Civ 028Документ9 страницCiv 028Deah RisbaОценок пока нет
- 2016 Article 1849 PDFДокумент8 страниц2016 Article 1849 PDFdydy_7193Оценок пока нет
- Dengue in Renal Transplant Patients A ReДокумент3 страницыDengue in Renal Transplant Patients A ReMaira EscobarОценок пока нет
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Документ6 страниц2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇAОценок пока нет
- Chakra - Factors Associated With Complications of C DiffДокумент8 страницChakra - Factors Associated With Complications of C DiffCherry SmileОценок пока нет
- Jorgensen 2017Документ6 страницJorgensen 2017jessicapxeОценок пока нет
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisДокумент8 страницChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiОценок пока нет
- Measures of Disease Frequency: Prevalence and IncidenceДокумент4 страницыMeasures of Disease Frequency: Prevalence and IncidenceVenia MursalimОценок пока нет
- Clinical and Laboratory Characteristics of Pediatric Dengue Fever Patients in A Tertiary Care HospitalДокумент4 страницыClinical and Laboratory Characteristics of Pediatric Dengue Fever Patients in A Tertiary Care HospitalPratiwi UmbohОценок пока нет
- The Clinical Spectrum of Henoch - Schönlein Purpura in Children: A Single-Center StudyДокумент8 страницThe Clinical Spectrum of Henoch - Schönlein Purpura in Children: A Single-Center StudyDaniela PetricanОценок пока нет
- Community-Acquired Pneumonia Requiring Hospitalization Among U.S. AdultsДокумент13 страницCommunity-Acquired Pneumonia Requiring Hospitalization Among U.S. AdultsCindy De PataОценок пока нет
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioДокумент7 страницThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniОценок пока нет
- 10 1016@j Jaad 2019 05 096Документ8 страниц10 1016@j Jaad 2019 05 096JohnОценок пока нет
- Diabetes With Hypertension As Risk Factors For Adult Dengue Hemorrhagic Fever in A Predominantly Dengue Serotype 2 Epidemic: A Case Control StudyДокумент12 страницDiabetes With Hypertension As Risk Factors For Adult Dengue Hemorrhagic Fever in A Predominantly Dengue Serotype 2 Epidemic: A Case Control StudyDwitari Novalia HaraziОценок пока нет
- Immunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary ReportДокумент9 страницImmunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary Reportrizki agusmaiОценок пока нет
- A Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesДокумент6 страницA Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesFelisiana KasmanОценок пока нет
- Lepto SpirosДокумент8 страницLepto SpirosNisa UcilОценок пока нет
- Idsa GuidelinesДокумент34 страницыIdsa GuidelinesROSEN NОценок пока нет
- Mathur 2015Документ7 страницMathur 2015Maximiliano OliveraОценок пока нет
- Complicaciones Neurológicas de Las Infecciones Por Rotavirus en Niños Ped Inf Dis 07 2023Документ4 страницыComplicaciones Neurológicas de Las Infecciones Por Rotavirus en Niños Ped Inf Dis 07 2023ANNIX FERRERОценок пока нет
- mdw557 2Документ7 страницmdw557 2mfaddhilОценок пока нет
- Tourniquet TestingДокумент6 страницTourniquet TestingPatrick RamosОценок пока нет
- Predictive Value of Proteinuria in Adult Dengue SeverityДокумент6 страницPredictive Value of Proteinuria in Adult Dengue SeverityWindy SuryaОценок пока нет
- Efficacy of Clinacanthus Nutans Extracts in PatientsДокумент7 страницEfficacy of Clinacanthus Nutans Extracts in Patientsconrad9richterОценок пока нет
- IDSA Nec FascДокумент34 страницыIDSA Nec FascShameen KhanОценок пока нет
- Diarrea en QuimioterapiaДокумент6 страницDiarrea en QuimioterapiaPaola DiazОценок пока нет
- 10.1007@s12098 020 03454 1Документ6 страниц10.1007@s12098 020 03454 1rayhantaswinОценок пока нет
- Management of Patients Suspected of Having Dengue FeverДокумент6 страницManagement of Patients Suspected of Having Dengue FeverRam Kripal MishraОценок пока нет
- Point-Of-Care Diagnostic Tests For Influenza in The Emergency DepartmentДокумент15 страницPoint-Of-Care Diagnostic Tests For Influenza in The Emergency DepartmentCristiano NogueiraОценок пока нет
- Menstrual Toxic Shock SyndromeДокумент9 страницMenstrual Toxic Shock SyndromeKristine MonicaОценок пока нет
- Etiology of Neonatal Sepsis in Five Urban Hospitals in The PhilippinesДокумент11 страницEtiology of Neonatal Sepsis in Five Urban Hospitals in The PhilippinesAlexandra Duque-DavidОценок пока нет
- Nej Mo A 0807381Документ12 страницNej Mo A 0807381Mildred MontОценок пока нет
- Maternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoДокумент8 страницMaternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoLola del carmen RojasОценок пока нет
- EA Davis,: E Coli, G Vaginalis) Salmo-Nella, Campylobacter) Streptococcus)Документ1 страницаEA Davis,: E Coli, G Vaginalis) Salmo-Nella, Campylobacter) Streptococcus)Khupe KafundaОценок пока нет
- Pi Is 1201971213002142Документ5 страницPi Is 1201971213002142melisaberlianОценок пока нет
- Community-Acquired Pneumonia Requiring Hospitalization Among U.S. ChildrenДокумент11 страницCommunity-Acquired Pneumonia Requiring Hospitalization Among U.S. ChildrenHanida Rahmah TaminОценок пока нет
- Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkДокумент8 страницAge-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkTony RobertsОценок пока нет
- Lovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialДокумент9 страницLovastatin For The Treatment of Adult Patients With Dengue: A Randomized, Double-Blind, Placebo-Controlled TrialBpmStfbОценок пока нет
- Hospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionДокумент7 страницHospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionadhitiaОценок пока нет
- Mortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsДокумент10 страницMortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsAdam PrabataОценок пока нет
- Microbiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemДокумент13 страницMicrobiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemJanatinAzaОценок пока нет
- Effect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyДокумент4 страницыEffect of Prednisolone During Defervescence in Dengue Haemorrhagic Fever: An Open Label Controlled StudyFabiola StellaОценок пока нет
- Current Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatesДокумент8 страницCurrent Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatespaulaveronicaОценок пока нет
- Christensen 2020Документ11 страницChristensen 2020Francisco ChourioОценок пока нет
- Kumar 2006Документ8 страницKumar 2006aiturraldeОценок пока нет
- Jose Research v2Документ10 страницJose Research v2Jose Emmanuel FranciaОценок пока нет
- 6 - Iype2014Документ7 страниц6 - Iype2014Muhammad SyaifullahОценок пока нет
- Zhang 2019 Plos NTDДокумент20 страницZhang 2019 Plos NTDlibremdОценок пока нет
- Questions To Integrate A Gender Perspective Into Research CooperationДокумент3 страницыQuestions To Integrate A Gender Perspective Into Research CooperationlibremdОценок пока нет
- Cloete 2018 Scielo South AfricaДокумент10 страницCloete 2018 Scielo South AfricalibremdОценок пока нет
- Curriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EduДокумент34 страницыCurriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EdulibremdОценок пока нет
- Boukary 2012 Plos OneДокумент12 страницBoukary 2012 Plos OnelibremdОценок пока нет
- Tesis AlirezaДокумент98 страницTesis AlirezalibremdОценок пока нет
- Arnault 2008 Is There An Asian Idiom of Distress Somatic Symptoms in FemaleДокумент15 страницArnault 2008 Is There An Asian Idiom of Distress Somatic Symptoms in FemalelibremdОценок пока нет
- Multinomial Logistic Regression Basic RelationshipsДокумент73 страницыMultinomial Logistic Regression Basic RelationshipslibremdОценок пока нет
- No Woman Should Die Giving LifeДокумент112 страницNo Woman Should Die Giving LifelibremdОценок пока нет
- Nutrition Transition in 2 Lowland Bolivian Subsistence PopulationsДокумент13 страницNutrition Transition in 2 Lowland Bolivian Subsistence PopulationslibremdОценок пока нет
- Call For Abstracts Social Inequity in Health SymposiumДокумент1 страницаCall For Abstracts Social Inequity in Health SymposiumlibremdОценок пока нет
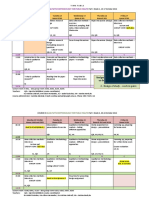
- QM 1 Schedule 2014-15 Final 0930 CambroДокумент2 страницыQM 1 Schedule 2014-15 Final 0930 CambrolibremdОценок пока нет
- Cineforum 2017: Director: Davis GuggenheimДокумент1 страницаCineforum 2017: Director: Davis GuggenheimlibremdОценок пока нет
- Clinical Dementia Rating Worksheet: Memory Questions For InformantДокумент10 страницClinical Dementia Rating Worksheet: Memory Questions For InformantlibremdОценок пока нет
- Welcomeletter Research Method and Philosophy November 2014Документ1 страницаWelcomeletter Research Method and Philosophy November 2014libremdОценок пока нет
- Fahetal2010 PDFДокумент10 страницFahetal2010 PDFlibremdОценок пока нет
- Abstract Book Leish World Congress 5Документ1 116 страницAbstract Book Leish World Congress 5libremdОценок пока нет
- Borang IshipДокумент9 страницBorang IshipUlfa RahayuОценок пока нет
- 5000L Series CatalogueДокумент24 страницы5000L Series CataloguekahlaouiОценок пока нет
- Assessing Health Impacts of Air Pollution From Electricity Generation The Case of ThailandДокумент22 страницыAssessing Health Impacts of Air Pollution From Electricity Generation The Case of Thailandcamilo_ortiz_6100% (1)
- Alumec 89 DatabladДокумент12 страницAlumec 89 DatabladMedoBoudyОценок пока нет
- 10 Suresh Nair - Journey ManagementДокумент25 страниц10 Suresh Nair - Journey ManagementMuhammad Zulkifli HarahapОценок пока нет
- Starbucks Managing High Growth BrandДокумент15 страницStarbucks Managing High Growth BrandSumit BansalОценок пока нет
- Week 5 UltrasoundДокумент26 страницWeek 5 UltrasoundNoor FarhanОценок пока нет
- Roth Conversion Strategies To ConsiderДокумент5 страницRoth Conversion Strategies To Considerkj4892Оценок пока нет
- Upstream Marine Standard IBU ChevronДокумент52 страницыUpstream Marine Standard IBU ChevronAndrew Hendy Indrakusuma50% (2)
- CUP 04 BOIN USA 02 WebДокумент2 страницыCUP 04 BOIN USA 02 WebMajid abdulОценок пока нет
- Brammer Standard Company, Inc.: Bs Su LAS-14Документ3 страницыBrammer Standard Company, Inc.: Bs Su LAS-14Ali MohsinОценок пока нет
- Unit 1 - 2Документ3 страницыUnit 1 - 2BahrouniОценок пока нет
- LabreportДокумент4 страницыLabreportDarwinys SamijonОценок пока нет
- Transcritical Co2 Refrigeration - PDFДокумент11 страницTranscritical Co2 Refrigeration - PDFHector Fabian Hernandez Algarra100% (1)
- Toyota/Lexus U140E/F, U240E, U241E: Click On Part Numbers For Product Details or VisitДокумент1 страницаToyota/Lexus U140E/F, U240E, U241E: Click On Part Numbers For Product Details or Visitvipper king2012Оценок пока нет
- Formatof Indenity BondДокумент2 страницыFormatof Indenity BondSudhir SinhaОценок пока нет
- Zuckerindustrie 139 (2) - 2014Документ9 страницZuckerindustrie 139 (2) - 2014Mateus RochaОценок пока нет
- People. Passion. Possibilities.: .30 .11 Thread Relief As RequiredДокумент40 страницPeople. Passion. Possibilities.: .30 .11 Thread Relief As RequiredFranciscoОценок пока нет
- United States Patent: (45) Date of Patent: Sep - 8, 2020Документ14 страницUnited States Patent: (45) Date of Patent: Sep - 8, 2020M FОценок пока нет
- LOTO-100 CompactoДокумент3 страницыLOTO-100 CompactoRyan KaneОценок пока нет
- Final - Urban and Transportation Engineering - PPT Group 1Документ19 страницFinal - Urban and Transportation Engineering - PPT Group 1JayChristian QuimsonОценок пока нет
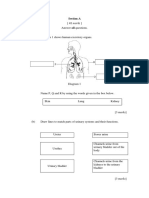
- Section A: Jawab Semua SoalanДокумент3 страницыSection A: Jawab Semua SoalanAzreen IzetОценок пока нет
- RFOC Learner's Guide Page 1-212Документ240 страницRFOC Learner's Guide Page 1-212Travel GnrOneОценок пока нет
- Recent Advances in Natural Polymer-Based Drug Delivery SystemsДокумент18 страницRecent Advances in Natural Polymer-Based Drug Delivery SystemsTelmoОценок пока нет
- Metrel D.D. - Class A Power Quality AnalysersДокумент7 страницMetrel D.D. - Class A Power Quality AnalysersMonster LifeОценок пока нет
- Hydraulics A320Документ101 страницаHydraulics A320KamalVirk100% (6)
- More Evidence Confirms Diet's Link To Mental Health: Could An Apple A Day Really Keep Depression and Anxiety Away?Документ5 страницMore Evidence Confirms Diet's Link To Mental Health: Could An Apple A Day Really Keep Depression and Anxiety Away?psychologyconceptsОценок пока нет
- Sigma MP 102 (US) EN SdsДокумент9 страницSigma MP 102 (US) EN SdsEduardo GarzaОценок пока нет
- ScimagojrДокумент1 653 страницыScimagojrKomariah ErvitaОценок пока нет
- Sentence PatternДокумент2 страницыSentence PatternBrito RajОценок пока нет