Вам также может понравиться
- RC Circuits: Study Frequency Response of FiltersДокумент11 страницRC Circuits: Study Frequency Response of Filters2456903Оценок пока нет
- Chapter 1 Basics of Power System Part 1 42 PDFДокумент18 страницChapter 1 Basics of Power System Part 1 42 PDFshaik jaheerОценок пока нет
- The Prevention and Control of Part 5Документ5 страницThe Prevention and Control of Part 5Sopna BalakrishnanОценок пока нет
- Commutation ChokesДокумент10 страницCommutation Chokestudor_x27Оценок пока нет
- Early Radio Receivers, Called Crystal Radios, Used A "Cat's Whisker" of Fine Wire Pressing On A Crystal ofДокумент4 страницыEarly Radio Receivers, Called Crystal Radios, Used A "Cat's Whisker" of Fine Wire Pressing On A Crystal ofPoonam bhavsarОценок пока нет
- The InductorДокумент67 страницThe Inductorleonard1971Оценок пока нет
- What Is Step and Touch Potential and Reducing Resistance To Ground - E S GroundingДокумент10 страницWhat Is Step and Touch Potential and Reducing Resistance To Ground - E S GroundingsekaranОценок пока нет
- About Power FactorДокумент9 страницAbout Power Factorcjtagaylo100% (1)
- Electrical IeeeДокумент8 страницElectrical IeeeHarsha VardhanОценок пока нет
- Chpt11 1Документ23 страницыChpt11 1WESTLY JUCOОценок пока нет
- Rectifier - 1 Half-Wave Rectification - 2 Full-Wave Rectification - Peak Loss - The Full-Wave Bridge - RectifierДокумент9 страницRectifier - 1 Half-Wave Rectification - 2 Full-Wave Rectification - Peak Loss - The Full-Wave Bridge - Rectifierysn_usmaniОценок пока нет
- Tech Note 5Документ4 страницыTech Note 5Rakesh GudalaОценок пока нет
- AC Notes1Документ12 страницAC Notes1Varun ChaudharyОценок пока нет
- Inspection and Testing of Electrical InstallationДокумент8 страницInspection and Testing of Electrical InstallationKamugasha KagonyeraОценок пока нет
- Distance Protection PerformanceДокумент5 страницDistance Protection PerformanceabohamamОценок пока нет
- ESD Basics: Basic Concepts in Electrostatic Discharge (Esd)Документ27 страницESD Basics: Basic Concepts in Electrostatic Discharge (Esd)bayu ajiiОценок пока нет
- LED Strip Light Power Supply CalculatorДокумент3 страницыLED Strip Light Power Supply CalculatorNadeem Muhammad NadzОценок пока нет
- Residual Currrent DevicesДокумент24 страницыResidual Currrent DevicespgcedzovОценок пока нет
- 7 MicrogridsДокумент191 страница7 MicrogridsibtihalislamОценок пока нет
- PE Lab 08Документ4 страницыPE Lab 08Haseeb BalochОценок пока нет
- Principles of Power QualityДокумент4 страницыPrinciples of Power Qualitykartheek427Оценок пока нет
- Electrical SafetyДокумент47 страницElectrical SafetyNo Hope100% (1)
- Ramsey 2011 Provocative Theory 1Документ16 страницRamsey 2011 Provocative Theory 1Rosie BiltonОценок пока нет
- Principles and testing methods of earth ground resistanceДокумент85 страницPrinciples and testing methods of earth ground resistanceJack MbrehОценок пока нет
- Cts and Vts TheoryДокумент20 страницCts and Vts Theorymvpradeep87Оценок пока нет
- Grounded ResearchДокумент45 страницGrounded ResearchDan Lhery Susano GregoriousОценок пока нет
- Electrical HazardsДокумент50 страницElectrical HazardsKenneth CortezОценок пока нет
- Poor Grounding Contributes To Downtime But A Lack of Good Grounding Is Also Dangerous and Increases The Risk of Equipment FailureДокумент5 страницPoor Grounding Contributes To Downtime But A Lack of Good Grounding Is Also Dangerous and Increases The Risk of Equipment FailureSTG INSTRUMENTОценок пока нет
- EMF ExposureДокумент15 страницEMF ExposureSyieda ZamryОценок пока нет
- SurgeprotectionДокумент2 страницыSurgeprotectionJohn Tristan100% (1)
- Microgrid Testbeds Around the World: A Review of Distributed Energy SystemsДокумент22 страницыMicrogrid Testbeds Around the World: A Review of Distributed Energy SystemsfawadazeemqaisraniОценок пока нет
- Hydrogen Fuel Cell BasicsДокумент9 страницHydrogen Fuel Cell BasicsAli SamОценок пока нет
- IEEE PES Power & Energy Society: Benefits and PublicationsДокумент9 страницIEEE PES Power & Energy Society: Benefits and PublicationsTania TorresОценок пока нет
- Power QualityДокумент13 страницPower QualityBochiОценок пока нет
- Safety in Low Voltage Installations, Vol-2 Selection and Application of LV Protective DevicesДокумент103 страницыSafety in Low Voltage Installations, Vol-2 Selection and Application of LV Protective DevicesUET MAINОценок пока нет
- Transistor Tutorial: Bipolar vs FETДокумент4 страницыTransistor Tutorial: Bipolar vs FETlosmilzoОценок пока нет
- Transient Suppression Devices and PrinciplesДокумент8 страницTransient Suppression Devices and Principleskunalbhavsar1Оценок пока нет
- Faults and Defects in Power Transformers PDFДокумент4 страницыFaults and Defects in Power Transformers PDFipraoОценок пока нет
- Types of TransformersДокумент10 страницTypes of Transformersghazal hammam100% (2)
- Discipline Planning Organizing Managing Resources Program ManagementДокумент18 страницDiscipline Planning Organizing Managing Resources Program ManagementRajiv PuttОценок пока нет
- Grounding Principles The Need To Ground: European American AustralianДокумент10 страницGrounding Principles The Need To Ground: European American Australianprasannakumar_rajaОценок пока нет
- Developing A Global Interconnected Power System ModelДокумент14 страницDeveloping A Global Interconnected Power System ModelucetkalОценок пока нет
- Power Quality ManagementДокумент13 страницPower Quality ManagementAniruddh NagaОценок пока нет
- Ieee PapersДокумент8 страницIeee PapersAtit PatelОценок пока нет
- DC to AC Conversion Using InvertersДокумент24 страницыDC to AC Conversion Using InvertersABHISHEK KUMARОценок пока нет
- Transformers: Types and Classifications in 40 CharactersДокумент16 страницTransformers: Types and Classifications in 40 CharactersTahamee SHAIKHОценок пока нет
- Intro To Power Quality LEZNCHARLДокумент45 страницIntro To Power Quality LEZNCHARLLucas De MeloОценок пока нет
- Full WaveДокумент17 страницFull WaveSandeep KumarОценок пока нет
- Green Hydrogen Energy Fuel For The Future in IndiaДокумент6 страницGreen Hydrogen Energy Fuel For The Future in IndiaResearch ParkОценок пока нет
- DC DC ConvertorДокумент11 страницDC DC ConvertorJyothiОценок пока нет
- ECE Capstone Design Project on Renewable Energy DC-DC Converter ControlДокумент19 страницECE Capstone Design Project on Renewable Energy DC-DC Converter ControlSabir VeОценок пока нет
- Bipolar Transistor Basics ExplainedДокумент21 страницаBipolar Transistor Basics ExplainedYashobhit SharmaОценок пока нет
- Emission and Interaction from Domestic Installations in the Low Voltage Electricity NetworkДокумент158 страницEmission and Interaction from Domestic Installations in the Low Voltage Electricity Networkrobert_rjcОценок пока нет
- Frequency Response: 大同大學電機系 黃淑絹 副教授 schuang@ttu.edu.twДокумент88 страницFrequency Response: 大同大學電機系 黃淑絹 副教授 schuang@ttu.edu.tw葉士肇Оценок пока нет
- Biological Effects of Radiation (Physics)Документ13 страницBiological Effects of Radiation (Physics)Josiah Dave CalumpangОценок пока нет
- Stopping WW3: how to stop a Russian War escalating to World War IIIОт EverandStopping WW3: how to stop a Russian War escalating to World War IIIОценок пока нет
- Navarro - 2003Документ15 страницNavarro - 2003M Del Mar RosaОценок пока нет
- Residential and Occupational Exposure To 50 HZ Magnetic Fields and Malignant Melanoma: A Population Based StudyДокумент5 страницResidential and Occupational Exposure To 50 HZ Magnetic Fields and Malignant Melanoma: A Population Based StudyramachariОценок пока нет
- Radiation Measurement Phase 1 FinalДокумент29 страницRadiation Measurement Phase 1 FinalMichelle KhanОценок пока нет
- Dealing With Crosstalk in Electromagnetic Field Measurementsof Portable DevicesДокумент10 страницDealing With Crosstalk in Electromagnetic Field Measurementsof Portable Devicesdarko6102Оценок пока нет
- Electromagnetic Fields (EMF) Environmental Pollution and The MUOS CaseДокумент15 страницElectromagnetic Fields (EMF) Environmental Pollution and The MUOS CaseFiorenzo MarinelliОценок пока нет
- Effects of microwaves on peroxidase enzyme activityДокумент7 страницEffects of microwaves on peroxidase enzyme activityFiorenzo MarinelliОценок пока нет
- Exposure To 900 MHZ Electromagnetic Field Induces An Unbalance Between Pro-Apoptotic and Pro-Survival Signals in T-Lymphoblastoid Leukemia CCRF-CEM CellsДокумент9 страницExposure To 900 MHZ Electromagnetic Field Induces An Unbalance Between Pro-Apoptotic and Pro-Survival Signals in T-Lymphoblastoid Leukemia CCRF-CEM CellsFiorenzo MarinelliОценок пока нет
- Alteration of Enzymic Electron Transfer Reactions Induced by Microwaves Emitted by Mobile PhonesДокумент16 страницAlteration of Enzymic Electron Transfer Reactions Induced by Microwaves Emitted by Mobile PhonesFiorenzo MarinelliОценок пока нет
- Clinical Review - KEDRABДокумент97 страницClinical Review - KEDRABcoolchapОценок пока нет
- Esea Elementary and Secondary Education Act Outline CampionДокумент9 страницEsea Elementary and Secondary Education Act Outline Campionapi-340155293Оценок пока нет
- Dentwiton Company Profile (En) 20221019-V2.1Документ20 страницDentwiton Company Profile (En) 20221019-V2.1BRAIS FREIRÍA LORENZOОценок пока нет
- Operation and Maintenance of Power PlantДокумент31 страницаOperation and Maintenance of Power PlantAnkur Pathak100% (1)
- Ethics Case StudyДокумент5 страницEthics Case StudyCian MontefalcoОценок пока нет
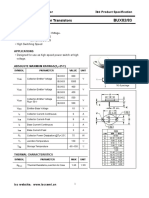
- Isc BUX82/83: Isc Silicon NPN Power TransistorsДокумент2 страницыIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCОценок пока нет
- SFNHS - Extension's School Learning Continuity PlanДокумент5 страницSFNHS - Extension's School Learning Continuity PlanClaudie MabiniОценок пока нет
- Lesson 5 Investigate Conditions Needed For GerminationДокумент12 страницLesson 5 Investigate Conditions Needed For GerminationJohany Gaona CruzОценок пока нет
- Notes Micro FinanceДокумент9 страницNotes Micro Financesofty1980Оценок пока нет
- Installation and Commissining of TransformerДокумент27 страницInstallation and Commissining of TransformereliahudОценок пока нет
- Laboratory Notebook: Aquatic Ecology and ResourcesДокумент7 страницLaboratory Notebook: Aquatic Ecology and ResourcesAireen Diamsim MaltoОценок пока нет
- Cherry Circle Room Main MenuДокумент8 страницCherry Circle Room Main MenuAshok SelvamОценок пока нет
- 7 HO Clearance Consent FormДокумент2 страницы7 HO Clearance Consent FormzanehfncbusinessОценок пока нет
- Gavekal PresentationДокумент35 страницGavekal PresentationFernando KlingОценок пока нет
- HVAC Control ModuleДокумент2 страницыHVAC Control ModuleData TécnicaОценок пока нет
- Energy EquationДокумент4 страницыEnergy EquationAnonymous VA3KeEwzОценок пока нет
- FP02BДокумент3 страницыFP02BRazak JeyОценок пока нет
- Efektivitas Penggunaan Komposit Polimer Yang Diperkuat Serat Untuk Perbaikan Pipa Baja Bawah AirДокумент15 страницEfektivitas Penggunaan Komposit Polimer Yang Diperkuat Serat Untuk Perbaikan Pipa Baja Bawah Air31Hanif ArdhioОценок пока нет
- 7 Mineral and Soil ResourcesДокумент21 страница7 Mineral and Soil ResourcesShardy Lyn RuizОценок пока нет
- Valve Manual Pocket EditionДокумент23 страницыValve Manual Pocket EditionBùi Cảnh Trung100% (1)
- Proton Pump Inhibitors v3Документ5 страницProton Pump Inhibitors v3shwampaОценок пока нет
- 3G3EV Installation ManualДокумент55 страниц3G3EV Installation ManualHajrudin SinanovićОценок пока нет
- Testing and Adjusting 12GДокумент5 страницTesting and Adjusting 12GJuan GonzalezОценок пока нет
- CHEMIST LICENSURE EXAM TABLEДокумент8 страницCHEMIST LICENSURE EXAM TABLEJasmin NewОценок пока нет
- Capstone PresentationДокумент19 страницCapstone PresentationArun BalachandranОценок пока нет
- Elo TecДокумент2 страницыElo TecMimi MimiОценок пока нет
- 2018-06-21 Calvert County TimesДокумент24 страницы2018-06-21 Calvert County TimesSouthern Maryland OnlineОценок пока нет
- l3 Muscle Physiology I 201920 2Документ6 страницl3 Muscle Physiology I 201920 2ARYSSA BINTI AZRIОценок пока нет
- Sisal FiberДокумент20 страницSisal FiberFahad juttОценок пока нет
- Barrioquinto vs. FernandezДокумент2 страницыBarrioquinto vs. FernandezIrene RamiloОценок пока нет