Вам также может понравиться
- Presentation 2Документ43 страницыPresentation 2talaarar695Оценок пока нет
- Pcos - Clinical Case DiscussionДокумент4 страницыPcos - Clinical Case Discussionreham macadatoОценок пока нет
- Different Faces of PCOS (Polycystic Ovarian Syndrome) : Shahnaz AkbarДокумент38 страницDifferent Faces of PCOS (Polycystic Ovarian Syndrome) : Shahnaz AkbararyОценок пока нет
- Polycystic Ovarian SyndromeДокумент20 страницPolycystic Ovarian SyndromeMuhammad khairul afizal RohimОценок пока нет
- Understanding Polycystic Ovarian SyndromeДокумент46 страницUnderstanding Polycystic Ovarian SyndromeStalin ChandrasekaranОценок пока нет
- PCOSДокумент38 страницPCOSJitendra ChaudharyОценок пока нет
- PCOS DR BasimaДокумент18 страницPCOS DR BasimaA.H.AОценок пока нет
- pcosДокумент9 страницpcosMonomay HalderОценок пока нет
- Polycystic Ovarian SyndromeДокумент17 страницPolycystic Ovarian SyndromeAhmed ElmohandesОценок пока нет
- PCOS-Epidemiology, Pathogenesis, Clinical Manifestations, Diagnosis and ManagementДокумент66 страницPCOS-Epidemiology, Pathogenesis, Clinical Manifestations, Diagnosis and ManagementAseel wael alshareefОценок пока нет
- Pcos 170123144542Документ86 страницPcos 170123144542Dewi Puspita Apsari100% (2)
- Polycystic Ovarian Syndrome (PCOS)Документ119 страницPolycystic Ovarian Syndrome (PCOS)Jasani JayrajОценок пока нет
- Hyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceДокумент7 страницHyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceNathan JeffreyОценок пока нет
- Physiotherapy in PCOSДокумент54 страницыPhysiotherapy in PCOSAkshaya Nayak100% (3)
- Polycystic Ovarian Syndrome (PCOSДокумент15 страницPolycystic Ovarian Syndrome (PCOSirfanОценок пока нет
- Untitled PDFДокумент2 страницыUntitled PDFGehad SalehОценок пока нет
- PCOS Review: Diagnosis, Treatment, ComorbiditiesДокумент3 страницыPCOS Review: Diagnosis, Treatment, ComorbiditiesJeremy LickteigОценок пока нет
- PCOS Signs and Symptoms GuideДокумент66 страницPCOS Signs and Symptoms GuidedenekeОценок пока нет
- Polycystic Ovarian Syndrome (PCOS)Документ57 страницPolycystic Ovarian Syndrome (PCOS)Michelle FynesОценок пока нет
- Polycystic Ovarian SyndromeДокумент2 страницыPolycystic Ovarian SyndromeCarlo CruzОценок пока нет
- Polycystic Ovary Syndrome: Dr. Rizwana ShaheenДокумент34 страницыPolycystic Ovary Syndrome: Dr. Rizwana ShaheenAmaan Hakim100% (1)
- Polcystic Ovarian SyndromeДокумент9 страницPolcystic Ovarian SyndromeMelissa BrodoОценок пока нет
- Managing PCOS with lifestyle changes and medicationsДокумент3 страницыManaging PCOS with lifestyle changes and medicationsSudeep GadhiyaОценок пока нет
- Polycystic Ovarian Syndrome: Dr. PrabhavathiДокумент30 страницPolycystic Ovarian Syndrome: Dr. PrabhavathiKasi PrasadОценок пока нет
- Polycystic Ovary SyndromeДокумент5 страницPolycystic Ovary SyndromeAle W.S.Оценок пока нет
- My PCOSДокумент54 страницыMy PCOSanees_aneessОценок пока нет
- Womens HealthДокумент12 страницWomens HealthPooja ChoudharyОценок пока нет
- Polycystic Ovary Syndrome (PCOS) Factsheet: Key PointsДокумент3 страницыPolycystic Ovary Syndrome (PCOS) Factsheet: Key PointsrhaineОценок пока нет
- Ovario Poliquístico/Polycystic Ovary SyndromeДокумент14 страницOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- Polycystic Ovary Syndrome: Under Supervision ofДокумент7 страницPolycystic Ovary Syndrome: Under Supervision ofHend HamedОценок пока нет
- PCO Road MapДокумент66 страницPCO Road MapDr. Rajul TyagiОценок пока нет
- Hirsutism: Diagnosis and TreatmentДокумент6 страницHirsutism: Diagnosis and TreatmentAnonymous ysrxggk21cОценок пока нет
- MENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTДокумент36 страницMENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTAkinbani MoyosoreОценок пока нет
- Polycystic Ovary Syndrome (PCOS) : February 2020Документ5 страницPolycystic Ovary Syndrome (PCOS) : February 2020Lia MeivianeОценок пока нет
- What Causes Polycystic Ovarian Syndrome (PCOS) ?: Infertility Menstrual IrregularitiesДокумент8 страницWhat Causes Polycystic Ovarian Syndrome (PCOS) ?: Infertility Menstrual IrregularitiesdnllkzaОценок пока нет
- Chapter+27+the+Polycystic+Ovary+SyndromeДокумент4 страницыChapter+27+the+Polycystic+Ovary+Syndromepmj050gpОценок пока нет
- Polycystic OvaryДокумент25 страницPolycystic OvaryAli AbdElnaby SalimОценок пока нет
- PCOS and Lactation: Kristina Chamberlain, CNM, ARNP, IBCLCДокумент42 страницыPCOS and Lactation: Kristina Chamberlain, CNM, ARNP, IBCLCJayantiОценок пока нет
- Polycystic Ovarian SyndromeДокумент47 страницPolycystic Ovarian SyndromeAnonymous HgX3mN1o100% (1)
- Document 5Документ15 страницDocument 5SamОценок пока нет
- Clinical Picture of pcosWPS OfficeДокумент11 страницClinical Picture of pcosWPS OfficeEsraa SalemОценок пока нет
- Secamenhyper 120208102817 Phpapp02Документ31 страницаSecamenhyper 120208102817 Phpapp02Mohan DassОценок пока нет
- Pcod Natural TreatmentДокумент4 страницыPcod Natural Treatmenttusharphale100% (1)
- Polycystic Ovarian Syndrome Protocol Carson Newman College Courtney ConnollyДокумент7 страницPolycystic Ovarian Syndrome Protocol Carson Newman College Courtney ConnollycourtneyОценок пока нет
- PCOSДокумент3 страницыPCOSpravallikakvОценок пока нет
- 1519 - 105 - 1 - Polycystic Ovarian Syndrome Characteristics ControДокумент41 страница1519 - 105 - 1 - Polycystic Ovarian Syndrome Characteristics ControWael GaberОценок пока нет
- PCOS Facts: Understanding the Causes, Symptoms and Treatments of Polycystic Ovarian SyndromeДокумент18 страницPCOS Facts: Understanding the Causes, Symptoms and Treatments of Polycystic Ovarian SyndromeRahul AgarwalОценок пока нет
- Menstruation Related Disorders 1Документ41 страницаMenstruation Related Disorders 1tokosepedakentenlautОценок пока нет
- Pi Pcos Update-2022 230717 221503Документ7 страницPi Pcos Update-2022 230717 221503PeterОценок пока нет
- Acog Pcos PDFДокумент3 страницыAcog Pcos PDFJoanne BlancoОценок пока нет
- Therapeutic Success in The Primary Amenorrhea Is Very Limited. Management Is Done According To CauseДокумент66 страницTherapeutic Success in The Primary Amenorrhea Is Very Limited. Management Is Done According To CauseNyshan KarkiОценок пока нет
- MBBS-3 Ma015412Документ71 страницаMBBS-3 Ma015412diphylleia90grayiОценок пока нет
- PCODДокумент76 страницPCODShreyance Parakh100% (1)
- PCOSДокумент17 страницPCOSSmz ZainabОценок пока нет
- AmenorrheaДокумент40 страницAmenorrheaMeraol HusseinОценок пока нет
- Dark Green Vintage Minimalist Aesthetic Newspaper Fashion Marketing Ad Instagram StoryДокумент4 страницыDark Green Vintage Minimalist Aesthetic Newspaper Fashion Marketing Ad Instagram StoryJana Emery SumagangОценок пока нет
- Polycystic Ovary SyndromeДокумент17 страницPolycystic Ovary SyndromeramsaybajjuОценок пока нет
- سمنر نسائيهДокумент20 страницسمنر نسائيهsuad aliОценок пока нет
- Bpj12 Polycystic Pages 7-13Документ0 страницBpj12 Polycystic Pages 7-13Kimsha ConcepcionОценок пока нет
- How to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)От EverandHow to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)Рейтинг: 3.5 из 5 звезд3.5/5 (6)
- Gynaecological Laproscopy: By: DR - Hanaa Al-HeideryДокумент22 страницыGynaecological Laproscopy: By: DR - Hanaa Al-Heideryzianab aliОценок пока нет
- Gynaecological Laproscopy: By: DR - Hanaa Al-HeideryДокумент22 страницыGynaecological Laproscopy: By: DR - Hanaa Al-Heideryzianab aliОценок пока нет
- D&C Procedure GuideДокумент22 страницыD&C Procedure Guidezianab aliОценок пока нет
- Primary and Secondary Anenorrhea 2016-2017Документ24 страницыPrimary and Secondary Anenorrhea 2016-2017zianab ali100% (1)
- Physiology of The Menstrual CycleДокумент17 страницPhysiology of The Menstrual Cyclezianab aliОценок пока нет
- Contraception Part 2Документ13 страницContraception Part 2zianab aliОценок пока нет
- Contraception Part1Документ38 страницContraception Part1zianab aliОценок пока нет
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyДокумент11 страницContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliОценок пока нет
- Female Genital Tract Anatomy 5th YearДокумент12 страницFemale Genital Tract Anatomy 5th Yearzianab aliОценок пока нет
- 1 CervixДокумент12 страниц1 Cervixzianab aliОценок пока нет
- 1 Female Lower Genital Tract InfectionДокумент14 страниц1 Female Lower Genital Tract Infectionzianab aliОценок пока нет
- Ectopic Pregnancy Part 1Документ37 страницEctopic Pregnancy Part 1zianab aliОценок пока нет
- Understanding miscarriage: causes, types, symptoms, and treatmentДокумент38 страницUnderstanding miscarriage: causes, types, symptoms, and treatmentzianab aliОценок пока нет
- Ectopic Pregnancy Part 2Документ42 страницыEctopic Pregnancy Part 2zianab aliОценок пока нет
- What Is The Difference Between and ?: Menopause PerimenopauseДокумент39 страницWhat Is The Difference Between and ?: Menopause Perimenopausezianab aliОценок пока нет
- Recurrent Abortion: Causes, Diagnosis and ManagementДокумент34 страницыRecurrent Abortion: Causes, Diagnosis and Managementzianab aliОценок пока нет
- Drapping Course at Iloilo Science and Tech UniversityДокумент2 страницыDrapping Course at Iloilo Science and Tech UniversityTrisha Marie Nalla TallodarОценок пока нет
- Ca 2016 37Документ36 страницCa 2016 37singh1699Оценок пока нет
- 0900 - 1078 - 00 C500 D5 (QSX15G8 With PCC2100) : Issue 01 20/02/06 Initial IssueДокумент2 страницы0900 - 1078 - 00 C500 D5 (QSX15G8 With PCC2100) : Issue 01 20/02/06 Initial IssueEdgar RamirezОценок пока нет
- 2010 VANOC Financial ReportДокумент28 страниц2010 VANOC Financial ReportBob MackinОценок пока нет
- Hamleys Passport Program All SizesДокумент4 страницыHamleys Passport Program All SizescitizenprintproОценок пока нет
- Workshop Safety RulesДокумент5 страницWorkshop Safety RulesMeggy VillanuevaОценок пока нет
- Racecar Engineering 2005 07 PDFДокумент100 страницRacecar Engineering 2005 07 PDFfreddyonnimiОценок пока нет
- Footjob at The Job FairДокумент23 страницыFootjob at The Job Fairsai vasaОценок пока нет
- Patrick Caton Test ResultsДокумент3 страницыPatrick Caton Test ResultsdeanОценок пока нет
- Awop ReadmeДокумент15 страницAwop ReadmesilenceindigoОценок пока нет
- GM TechLink 21 November 2022Документ9 страницGM TechLink 21 November 2022River OzОценок пока нет
- Popcap Games Keys and SerialsДокумент5 страницPopcap Games Keys and SerialsTerrance Thien45% (11)
- R-10 MK2 Rifle Instructions: Gun SafetyДокумент2 страницыR-10 MK2 Rifle Instructions: Gun SafetyFernando S.A.Оценок пока нет
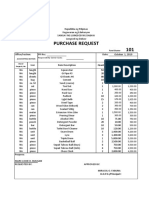
- 101 Purchase Request: Responsibility Center CodeДокумент1 страница101 Purchase Request: Responsibility Center CodeRosalie Cotillar BaldezamoОценок пока нет
- Tracheostomy Care Checklist 1Документ2 страницыTracheostomy Care Checklist 1Nicholas Tagle100% (2)
- Packing List For Jungle AdventureДокумент2 страницыPacking List For Jungle AdventureAlarik van Der IОценок пока нет
- The 2013 LEGO Minifigure CatalogДокумент9 страницThe 2013 LEGO Minifigure CatalogChristoph Bartneck100% (1)
- 6f50 TSB 4 PDFДокумент2 страницы6f50 TSB 4 PDFHumberto Lojan100% (2)
- Baseball Powerpoint Final Project 2Документ15 страницBaseball Powerpoint Final Project 2api-242139683Оценок пока нет
- AFC Club Ranking 2011-2014: Top 100 Clubs by PointsДокумент2 страницыAFC Club Ranking 2011-2014: Top 100 Clubs by PointsSuraedi TambakОценок пока нет
- C51B Start ListДокумент8 страницC51B Start ListCarmen AguilarОценок пока нет
- Target ShooterДокумент60 страницTarget Shooterdevildgog100% (1)
- TR-500E-3-00101 4 BOOM + 2 JIB, 2M2D PR1100026-02 TORQUE CONVERTERДокумент4 страницыTR-500E-3-00101 4 BOOM + 2 JIB, 2M2D PR1100026-02 TORQUE CONVERTERAries ApriliantoОценок пока нет
- Tees Hazari List of AdvocatesДокумент46 страницTees Hazari List of AdvocatesAnuj DulloОценок пока нет
- Icha MainanДокумент118 страницIcha Mainanrasah trial11Оценок пока нет
- Rifle Recoil ChartДокумент6 страницRifle Recoil Chartblowmeasshole1911Оценок пока нет
- PeriodisationДокумент17 страницPeriodisationBobОценок пока нет
- Troy Bilt MowerДокумент20 страницTroy Bilt MowerBob GinelОценок пока нет
- 21CH HospitalityBrochure PDFДокумент9 страниц21CH HospitalityBrochure PDFKyler RoseОценок пока нет
- We Are The WorldДокумент2 страницыWe Are The WorldSalma BondocОценок пока нет