Вам также может понравиться
- Assessing and Prognosing Pneumonia - DR DanielДокумент30 страницAssessing and Prognosing Pneumonia - DR Danielibrahim sengajiОценок пока нет
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiДокумент32 страницыThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianОценок пока нет
- 53224-ML-0843 Rev A The Next Stage in Cardiogenic Shock PPTДокумент23 страницы53224-ML-0843 Rev A The Next Stage in Cardiogenic Shock PPTjuancar90Оценок пока нет
- List of Critical and Panic ValuesДокумент2 страницыList of Critical and Panic Valuesdar alhikmahОценок пока нет
- Acep Evidencecare Covid19severitytoolДокумент3 страницыAcep Evidencecare Covid19severitytoolShariq IqbalОценок пока нет
- Emergency Department COVID-19 Severity ClassificationДокумент3 страницыEmergency Department COVID-19 Severity ClassificationAsti YumnaОценок пока нет
- Sepsis and Septic Shock: Definitions, Clinical Manifestations, and TreatmentДокумент9 страницSepsis and Septic Shock: Definitions, Clinical Manifestations, and TreatmentIan SabogalОценок пока нет
- Protocol For COVID-Management Updated Version 2.1 - AIIMS 3 May 2021Документ63 страницыProtocol For COVID-Management Updated Version 2.1 - AIIMS 3 May 2021Gopireddy Sivakarthik ReddyОценок пока нет
- Practical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingДокумент24 страницыPractical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingyusОценок пока нет
- Lit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCДокумент76 страницLit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCKomang_JananuragaОценок пока нет
- COVID TreatmentДокумент9 страницCOVID TreatmentMuhammad Saeed RazaОценок пока нет
- Screening ToolДокумент1 страницаScreening ToollucialОценок пока нет
- Guidelines Treatment Protocol April 2021 MergedДокумент78 страницGuidelines Treatment Protocol April 2021 Mergedjose j kochuparambilОценок пока нет
- Pneumonia Pathway Final 2010 Rev4Документ7 страницPneumonia Pathway Final 2010 Rev4lyuen600Оценок пока нет
- 2019 Copd OutpatientsДокумент61 страница2019 Copd OutpatientsArshamОценок пока нет
- EGDTДокумент33 страницыEGDTaLineLanОценок пока нет
- Sepsis: ManagementДокумент50 страницSepsis: Managementer bcmОценок пока нет
- Materi Presentasi Immune Response To Trauma & SIRS - SepsisДокумент27 страницMateri Presentasi Immune Response To Trauma & SIRS - SepsisYASMINDPОценок пока нет
- W2D3 DR - Yasa-Bacteremia Dan SepsisДокумент54 страницыW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviОценок пока нет
- Antivenom Reactions IntroductionДокумент14 страницAntivenom Reactions IntroductionppgpcsОценок пока нет
- Sepsis Management GuidelinesДокумент54 страницыSepsis Management Guidelinesfakhrina nur fadhillahОценок пока нет
- Sepsis in MalaysiaДокумент4 страницыSepsis in MalaysiaCaisha Nivenia MosesОценок пока нет
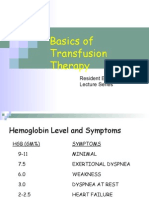
- Basics of Transfusion TherapyДокумент43 страницыBasics of Transfusion TherapyMuhammad Afyudin DjumhuriОценок пока нет
- Focused Clinical Case Study AssessmentДокумент32 страницыFocused Clinical Case Study AssessmentAndrea Isabel U. O'DellОценок пока нет
- Acute Pulmonary Embolism with DVT in 46-Year-Old Female PatientДокумент2 страницыAcute Pulmonary Embolism with DVT in 46-Year-Old Female PatientSO SОценок пока нет
- Homologous Blood Trasfusion Practice ShortsДокумент23 страницыHomologous Blood Trasfusion Practice ShortsdrprasadingleyОценок пока нет
- Thromboprophylaxis in Sepsis Case BasedДокумент32 страницыThromboprophylaxis in Sepsis Case BasedVasantha KumarОценок пока нет
- Covid-19 Initial Triaging & Case Management ProtocolДокумент24 страницыCovid-19 Initial Triaging & Case Management ProtocolDeepak SugumarОценок пока нет
- Predicting the Etiology of CLABSI: Bacterial vs Fungal InfectionsДокумент19 страницPredicting the Etiology of CLABSI: Bacterial vs Fungal InfectionssilviОценок пока нет
- Mis C Clinical GuidelineДокумент9 страницMis C Clinical GuidelineasyqarОценок пока нет
- Sepsis 3: As. Prof. Rotar OДокумент25 страницSepsis 3: As. Prof. Rotar OOleksandr RotarОценок пока нет
- CURB-65 A 7mmol (19mg/dl) BP 65: CURB-65, PSI, CPIS & AntibioticДокумент3 страницыCURB-65 A 7mmol (19mg/dl) BP 65: CURB-65, PSI, CPIS & AntibioticfaberОценок пока нет
- MiscДокумент29 страницMiscsam2000samОценок пока нет
- Guidelines On Management of Covid-19 Icu PatientДокумент32 страницыGuidelines On Management of Covid-19 Icu PatientBrainy LumineusОценок пока нет
- nsg-432 Careplan 2Документ11 страницnsg-432 Careplan 2api-521003884Оценок пока нет
- Translated document on pending BPJS claim verificationДокумент2 страницыTranslated document on pending BPJS claim verificationnovi rista anandaОценок пока нет
- CURB-65 Score For Pneumonia Score DescriptionДокумент14 страницCURB-65 Score For Pneumonia Score DescriptionMelvin CarewОценок пока нет
- Clinical Guideline For Management of Acute Cholecystitis in AdultsДокумент9 страницClinical Guideline For Management of Acute Cholecystitis in AdultsGaby D'LuneОценок пока нет
- Clinical Guideline For Management of Acute Cholecystitis in AdultsДокумент9 страницClinical Guideline For Management of Acute Cholecystitis in AdultsPutria Rezki ArgathyaОценок пока нет
- The PatientДокумент9 страницThe PatientJan Crizza Dale R. FrancoОценок пока нет
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungДокумент47 страницKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiОценок пока нет
- Surviving Sepsis: Early Goal Directed TherapyДокумент32 страницыSurviving Sepsis: Early Goal Directed Therapydr.mahensОценок пока нет
- FE ImbalanceДокумент6 страницFE ImbalanceDonna CortezОценок пока нет
- UPPER GI BLEED-finalДокумент81 страницаUPPER GI BLEED-finalMahendra PerumalОценок пока нет
- Screenshot 2020-03-20 at 08.25.44 PDFДокумент10 страницScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresОценок пока нет
- Management of Pneumonia: Criteria, Antibiotics, PreventionДокумент22 страницыManagement of Pneumonia: Criteria, Antibiotics, PreventionSeham AlsalamahОценок пока нет
- REVISED COVID-19 TREATMENT PROTOCOL - Version 3Документ17 страницREVISED COVID-19 TREATMENT PROTOCOL - Version 3abhishekОценок пока нет
- SEPSIS Early DetectionДокумент35 страницSEPSIS Early DetectionKomang_JananuragaОценок пока нет
- Referat Sepsis Dan ARDS - Lea SichiliaДокумент24 страницыReferat Sepsis Dan ARDS - Lea SichiliaLea SichiliaОценок пока нет
- Antibiotic Pocket GuideДокумент19 страницAntibiotic Pocket GuideNaomi Liang100% (1)
- 16 SepsisДокумент125 страниц16 SepsisChamindraОценок пока нет
- APRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEДокумент30 страницAPRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEAyen FornollesОценок пока нет
- 2019 LAMA For COPDДокумент25 страниц2019 LAMA For COPDdonnyОценок пока нет
- Dr. Sudarto Sppd's FileДокумент22 страницыDr. Sudarto Sppd's FileVindy CesarianaОценок пока нет
- City Hospitals Sunderland A&E Department: Information Card PackДокумент47 страницCity Hospitals Sunderland A&E Department: Information Card PackMulki HakamОценок пока нет
- GC Sepsis Apr 28 2013Документ31 страницаGC Sepsis Apr 28 2013Elys ElzОценок пока нет
- CSF Findings in MeningitisДокумент11 страницCSF Findings in MeningitisLioraОценок пока нет
- CAP by DR SarmaДокумент76 страницCAP by DR SarmaTina ReisaОценок пока нет
- UQU SLE CORRECTED FILE by DR Samina FidaДокумент537 страницUQU SLE CORRECTED FILE by DR Samina Fidaasma .sassi100% (1)
- Covid-19 Clinical PathwayДокумент7 страницCovid-19 Clinical Pathwayfatoma cheeseОценок пока нет
- writing مهم جدا PDFДокумент126 страницwriting مهم جدا PDFengy abdelrhimОценок пока нет
- Risks For Acute Respiratory Illnesses Score A. Exposure RisksДокумент1 страницаRisks For Acute Respiratory Illnesses Score A. Exposure Risksfatoma cheeseОценок пока нет
- Case Management 12-5-2020 PDFДокумент7 страницCase Management 12-5-2020 PDFfatoma cheeseОценок пока нет
- Adult electrolyte protocolsДокумент3 страницыAdult electrolyte protocolsRatih Dwi OctariaОценок пока нет
- Day Letter: Sample Test 1 Sample Test 2 OET Online 6 E2 Full Set 3 E2 Full Set 3 Adel Test 1 Oet Online 5 E2 Full Set 2Документ3 страницыDay Letter: Sample Test 1 Sample Test 2 OET Online 6 E2 Full Set 3 E2 Full Set 3 Adel Test 1 Oet Online 5 E2 Full Set 2fatoma cheeseОценок пока нет
- Training Project Proposal ERFSIДокумент10 страницTraining Project Proposal ERFSIfatoma cheeseОценок пока нет
- Covid Severity Scoring Tool PDFДокумент1 страницаCovid Severity Scoring Tool PDFfatoma cheeseОценок пока нет
- Coronavirus - No Panic Helpguide PDFДокумент30 страницCoronavirus - No Panic Helpguide PDFaasthakhannaОценок пока нет
- Case Management 12-5-2020 PDFДокумент7 страницCase Management 12-5-2020 PDFfatoma cheeseОценок пока нет
- Covid Severity Scoring Tool PDFДокумент1 страницаCovid Severity Scoring Tool PDFfatoma cheeseОценок пока нет
- Salter 2018 - Changes in Temperature Management of Cardiac Arrest Patients Following Publication of The Target Temperature Management TrialДокумент9 страницSalter 2018 - Changes in Temperature Management of Cardiac Arrest Patients Following Publication of The Target Temperature Management TrialSteven BrownОценок пока нет
- Mental Health Studyguide Part 1Документ39 страницMental Health Studyguide Part 1Ngoc TB VoОценок пока нет
- Nutrition Science: Online Short CourseДокумент10 страницNutrition Science: Online Short CourseVivekОценок пока нет
- Long Cases ABM ABDULLAH 1st Edition PDFДокумент844 страницыLong Cases ABM ABDULLAH 1st Edition PDFProthoma Dey64% (11)
- Activity 1. Introduction To Transcultural NursingДокумент7 страницActivity 1. Introduction To Transcultural NursingANAMAZING CHANNELОценок пока нет
- Knowledge, Attitude and Practices of School Children On Prevention and Control of Superficial Fungal in Western KenyaДокумент7 страницKnowledge, Attitude and Practices of School Children On Prevention and Control of Superficial Fungal in Western KenyaPremier PublishersОценок пока нет
- Nasm Study Guide PDF 2016 Nasm CPTДокумент54 страницыNasm Study Guide PDF 2016 Nasm CPTAlonzo Mark100% (7)
- Letters Abstract Proposed RP - LoveДокумент11 страницLetters Abstract Proposed RP - LoveoliviaОценок пока нет
- 1948 Staff Listing for PREPPO HospitalДокумент481 страница1948 Staff Listing for PREPPO Hospitalpriya selvarajОценок пока нет
- The Role of The Government in Economics: Executive SummaryДокумент10 страницThe Role of The Government in Economics: Executive SummaryrojithvОценок пока нет
- The Age of Anxiety: Baroque EclogueДокумент124 страницыThe Age of Anxiety: Baroque EclogueSatish100% (4)
- Role of Ophthalmic Nurses in Prevention of Ophthalmic DiseasesДокумент4 страницыRole of Ophthalmic Nurses in Prevention of Ophthalmic DiseaseskaskwawОценок пока нет
- Twin Flame Pain of Being Apart GuideДокумент5 страницTwin Flame Pain of Being Apart GuideShanneasy FlanОценок пока нет
- Material: Safety Data SheetДокумент3 страницыMaterial: Safety Data SheetMichael JoudalОценок пока нет
- Interventions For Preventing Falls in People After Stroke (Review)Документ68 страницInterventions For Preventing Falls in People After Stroke (Review)Abdelrhman AhmedОценок пока нет
- Chapter 1and2 JeepneydriversДокумент33 страницыChapter 1and2 JeepneydriversMarco LamanilaoОценок пока нет
- DFV Diagnostic Product Guide ResourceДокумент19 страницDFV Diagnostic Product Guide ResourceSer NdcОценок пока нет
- Hc3.1. Homeless Population: Definitions and MethodologyДокумент12 страницHc3.1. Homeless Population: Definitions and Methodologypaulscribd1Оценок пока нет
- Awesome: Toilet Training TipsДокумент3 страницыAwesome: Toilet Training TipsBindu SripadОценок пока нет
- Front Back: Adacium Rapid 50mg TabletsДокумент1 страницаFront Back: Adacium Rapid 50mg TabletsAmri MuharamОценок пока нет
- Tank Erection Risk Assessment - UTAMДокумент3 страницыTank Erection Risk Assessment - UTAMmohamed Abo-Ewisha100% (1)
- Jurnal 2Документ9 страницJurnal 2Rio ArdiantoruОценок пока нет
- Practice QuestionsДокумент24 страницыPractice QuestionsMonique RapleyОценок пока нет
- 1 Assessment Data Form MS-1Документ6 страниц1 Assessment Data Form MS-1alharbimanar20Оценок пока нет
- Vata RaktaДокумент27 страницVata RaktaKristina Babic100% (2)
- Stihl Ts 410 420 Owners Instruction ManualДокумент112 страницStihl Ts 410 420 Owners Instruction ManualLucyan IonescuОценок пока нет
- Home Economics-Household Services "Prepare Hot and Cold Meals/Food" Meal/ Food Preparation Week 2 (1 Quarter)Документ2 страницыHome Economics-Household Services "Prepare Hot and Cold Meals/Food" Meal/ Food Preparation Week 2 (1 Quarter)KISHAОценок пока нет
- Good Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesДокумент5 страницGood Clinical Laboratory Practice (GCLP) : Quality Demanding From Clinical LaboratoriesJaneОценок пока нет
- Clinical Case ConferenceДокумент22 страницыClinical Case ConferenceTallal BurwagОценок пока нет
- Comparing Anxiety and Clinical Success of Composites vs Colored CompomersДокумент7 страницComparing Anxiety and Clinical Success of Composites vs Colored CompomersRaul GhiurcaОценок пока нет