Вам также может понравиться
- Molar Incisor Hypomineralization A Literature ReviДокумент6 страницMolar Incisor Hypomineralization A Literature ReviAngie Figueroa OtaloraОценок пока нет
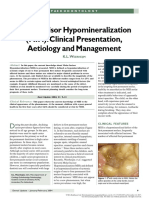
- Molar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementДокумент3 страницыMolar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementLaura MonáОценок пока нет
- Missing Links of Molar Incisor Hypomineralization: A ReviewДокумент11 страницMissing Links of Molar Incisor Hypomineralization: A ReviewShinta Dewi NОценок пока нет
- Molar Incisor Hypomineralization: Review and Recommendations For Clinical ManagementДокумент9 страницMolar Incisor Hypomineralization: Review and Recommendations For Clinical ManagementanonimoОценок пока нет
- Molar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementДокумент3 страницыMolar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementSelvaArockiamОценок пока нет
- Articulo en Ingles OdontopediatriaДокумент10 страницArticulo en Ingles OdontopediatriaAna Belén Escobar NoboaОценок пока нет
- Ameloblastic Fibro-Odontoma: A Case ReportДокумент4 страницыAmeloblastic Fibro-Odontoma: A Case Reportoral pathОценок пока нет
- A Complex Odontoma of The Anterior Maxilla AssociaДокумент5 страницA Complex Odontoma of The Anterior Maxilla AssociaJulka MadejОценок пока нет
- Sylwia Falkowska 2019.molar-Incisor Hypomineralisation (MIH) - Aetiology, Clinical Picture, TreatmentДокумент5 страницSylwia Falkowska 2019.molar-Incisor Hypomineralisation (MIH) - Aetiology, Clinical Picture, TreatmentMairen RamirezОценок пока нет
- Jnma 59 235 295Документ8 страницJnma 59 235 295Fabiola MartinezОценок пока нет
- 10 Muhammad Salman RashidДокумент3 страницы10 Muhammad Salman Rashidrahul sharmaОценок пока нет
- Molar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementДокумент4 страницыMolar Incisor Hypomineralization (MIH) : Clinical Presentation, Aetiology and ManagementAndreea Mihaela LazărОценок пока нет
- HypomineralizedSecondPrimaryMolar3 PDFДокумент4 страницыHypomineralizedSecondPrimaryMolar3 PDFnha khoa NHƯ NGỌCОценок пока нет
- Hypomin or HypoplasiaДокумент4 страницыHypomin or HypoplasiababukanchaОценок пока нет
- Ipdoaj MS Id 000113Документ3 страницыIpdoaj MS Id 000113Ayu DamayОценок пока нет
- Emergency Management of Temporomandibular Joint Dislocation With Manual ReductionДокумент5 страницEmergency Management of Temporomandibular Joint Dislocation With Manual ReductionRisallah CintaОценок пока нет
- Conservative ManagementДокумент4 страницыConservative ManagementFatima AliОценок пока нет
- Simultaneous Occurrence of Hypodontia and Microdontia in A Single CaseДокумент3 страницыSimultaneous Occurrence of Hypodontia and Microdontia in A Single CaseNadeemОценок пока нет
- Clasification of Odontogenic Tumours A ReviewДокумент6 страницClasification of Odontogenic Tumours A ReviewJuan Carlos MeloОценок пока нет
- Review of The Genetic Basis of Jaw Malformations: Mairaj K. Ahmed Xiaoqian Ye Peter J. TaubДокумент11 страницReview of The Genetic Basis of Jaw Malformations: Mairaj K. Ahmed Xiaoqian Ye Peter J. Taubchristian roblesОценок пока нет
- Odontoma Compound 1Документ4 страницыOdontoma Compound 1ashariОценок пока нет
- Orthodontics and Pediatric DentistryДокумент62 страницыOrthodontics and Pediatric DentistryAnggaHumalaBeltsazarNapitupuluОценок пока нет
- Long Face Syndrome: A Literature Review: Journal of Dental Health Oral Disorders & TherapyДокумент4 страницыLong Face Syndrome: A Literature Review: Journal of Dental Health Oral Disorders & TherapyGauri KhadeОценок пока нет
- GRUPO 4 HIM-Caries Americano 2017Документ11 страницGRUPO 4 HIM-Caries Americano 2017Vanessa MinОценок пока нет
- Sri Maya Koas 15 - 5 - Managemen AmelogenesisДокумент9 страницSri Maya Koas 15 - 5 - Managemen AmelogenesisMaya MunggaranОценок пока нет
- CA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleДокумент4 страницыCA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleThành Luân NguyễnОценок пока нет
- 2017 - Ameloblastic Fibroodontoma Uncommon Case Presentation in A 6 Year Old ChildДокумент4 страницы2017 - Ameloblastic Fibroodontoma Uncommon Case Presentation in A 6 Year Old ChildSyifa IKОценок пока нет
- Caso ClínicoДокумент3 страницыCaso ClínicoAbelОценок пока нет
- 4 Ads 16 112 PDFДокумент4 страницы4 Ads 16 112 PDFJeyachandran MariappanОценок пока нет
- Tooth Fusion-A Rare Dental Anomaly: Analysis of Six CasesДокумент5 страницTooth Fusion-A Rare Dental Anomaly: Analysis of Six CasessafutriОценок пока нет
- Case Report: Odontogenic Fibromyxoma of Maxilla: A Rare Case ReportДокумент5 страницCase Report: Odontogenic Fibromyxoma of Maxilla: A Rare Case ReportQurbaIlmuwanFirdausОценок пока нет
- Oral Pathology in Paediatric Patients-Mini-Systematic ReviewДокумент7 страницOral Pathology in Paediatric Patients-Mini-Systematic ReviewYuganya SriОценок пока нет
- Applsci 11 00004Документ13 страницApplsci 11 00004Ela LilyОценок пока нет
- Celulitis Odontogenica en Niños Caso Clinico 2Документ6 страницCelulitis Odontogenica en Niños Caso Clinico 2ana mariaОценок пока нет
- Manish PDFДокумент4 страницыManish PDFLeena Losheene VijayakumarОценок пока нет
- MesiodensДокумент1 страницаMesiodensSAGAR ADHIKARIОценок пока нет
- 3.tahrir N. Aldelaimi Article Bony Syngnathia (Congenital Fusion of Maxilla and Mandible)Документ3 страницы3.tahrir N. Aldelaimi Article Bony Syngnathia (Congenital Fusion of Maxilla and Mandible)Mohammed AbdulhammedОценок пока нет
- Guideline On Dental Management of Heritable Dental Developmental AnomaliesДокумент6 страницGuideline On Dental Management of Heritable Dental Developmental AnomaliesNicky MachareonsapОценок пока нет
- Gingival Pigmentation and Its Treatment ModalititesДокумент4 страницыGingival Pigmentation and Its Treatment ModalititesramaОценок пока нет
- Oral Melanotic Macule - An Unusual Occurrence in GingivaДокумент4 страницыOral Melanotic Macule - An Unusual Occurrence in GingivaYeni PuspitasariОценок пока нет
- Article-Etiology Enamel DefectsДокумент10 страницArticle-Etiology Enamel DefectsSteph Vázquez SuárezОценок пока нет
- Complications of An Unrecognized Cheek Biting Habit Following A Dental VisitДокумент3 страницыComplications of An Unrecognized Cheek Biting Habit Following A Dental VisitChintya Monica AmelindaОценок пока нет
- Ijpi 2 (2) 61-63Документ3 страницыIjpi 2 (2) 61-63Tiara HapkaОценок пока нет
- Pedodontics: Non Syndromic Familial Hypodontia - A Case SeriesДокумент6 страницPedodontics: Non Syndromic Familial Hypodontia - A Case SeriesGabriel LazarОценок пока нет
- Hemifacial Microsomia - by The Little Baby Face FoundationДокумент1 страницаHemifacial Microsomia - by The Little Baby Face FoundationThe Little Baby Face FoundationОценок пока нет
- Jurnal Resesi 6Документ4 страницыJurnal Resesi 6viena mutmainnahОценок пока нет
- Amelogenesis Imperfecta: Therapeutic Strategy From Primary To Permanent Dentition Across Case ReportsДокумент8 страницAmelogenesis Imperfecta: Therapeutic Strategy From Primary To Permanent Dentition Across Case ReportsbanyubiruОценок пока нет
- Oral and Maxillofacial PathologyДокумент11 страницOral and Maxillofacial PathologyIzadora VeigaОценок пока нет
- Class I Angle Penjelasan Ama DisertainyaДокумент6 страницClass I Angle Penjelasan Ama Disertainyahtpxol1Оценок пока нет
- Ijdr 201723 01Документ3 страницыIjdr 201723 01lily oktarizaОценок пока нет
- Caser Report PDFДокумент4 страницыCaser Report PDFNabil AlkaffОценок пока нет
- William2 28 3Документ9 страницWilliam2 28 3Mirela TomaОценок пока нет
- Manjunatha BS, 2015Документ3 страницыManjunatha BS, 2015Bruna FerreiraОценок пока нет
- Amelogenesis Imperfecta and Anterior Open Bite: Etiological, Classification, Clinical and Management InterrelationshipsДокумент6 страницAmelogenesis Imperfecta and Anterior Open Bite: Etiological, Classification, Clinical and Management InterrelationshipsMelisa GuerraОценок пока нет
- Amelogenesis Imperfecta: Review of Diagnostic Findings and Treatment ConceptsДокумент12 страницAmelogenesis Imperfecta: Review of Diagnostic Findings and Treatment ConceptsBruno M. StrangioОценок пока нет
- Best Clinical Practice Guidance For Clinicians Dealing With Children Presenting With Molar-Incisor-Hypomineralisation (MIH)Документ7 страницBest Clinical Practice Guidance For Clinicians Dealing With Children Presenting With Molar-Incisor-Hypomineralisation (MIH)Fernanda Vicioni MarquesОценок пока нет
- Guideline DiДокумент6 страницGuideline DiBoris ChapelletОценок пока нет
- Article DentureStomatitis AReviewДокумент7 страницArticle DentureStomatitis AReviewSkAliHassanОценок пока нет
- Down Syndrome Associated To Periodontitis. A Review.Документ7 страницDown Syndrome Associated To Periodontitis. A Review.María Jesús EspínolaОценок пока нет
- Dental Education: Oral Health Behaviour and Awareness of Young Population in TurkeyДокумент7 страницDental Education: Oral Health Behaviour and Awareness of Young Population in TurkeyGabriel LazarОценок пока нет
- An Evidence-Based Reference: Diseases and Conditions in DentistryДокумент1 страницаAn Evidence-Based Reference: Diseases and Conditions in DentistryGabriel LazarОценок пока нет
- Article 6 1 2Документ6 страницArticle 6 1 2Gabriel LazarОценок пока нет
- Article 6 1 6Документ12 страницArticle 6 1 6Gabriel LazarОценок пока нет
- Book Rev 6 1 5Документ1 страницаBook Rev 6 1 5Gabriel LazarОценок пока нет
- Concepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIДокумент1 страницаConcepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIGabriel Lazar100% (1)
- Article 5 3 4Документ7 страницArticle 5 3 4Gabriel LazarОценок пока нет
- Dental Materials: Effects of Etching Mode On Bond Strength of Universal AdhesivesДокумент7 страницDental Materials: Effects of Etching Mode On Bond Strength of Universal AdhesivesGabriel LazarОценок пока нет
- Article 5 3 3Документ9 страницArticle 5 3 3Gabriel LazarОценок пока нет
- Concepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIДокумент1 страницаConcepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIGabriel Lazar100% (1)
- Article 6 1 3 PDFДокумент5 страницArticle 6 1 3 PDFGabriel LazarОценок пока нет
- Article 6 1 1 PDFДокумент9 страницArticle 6 1 1 PDFGabriel LazarОценок пока нет
- Article 6 2 6Документ9 страницArticle 6 2 6Gabriel LazarОценок пока нет
- Article 6 2 2Документ11 страницArticle 6 2 2Gabriel LazarОценок пока нет
- Dental Materials: in Vitro Wear of Ten Universal CompositesДокумент9 страницDental Materials: in Vitro Wear of Ten Universal CompositesGabriel LazarОценок пока нет
- BookRev 5 2 5Документ1 страницаBookRev 5 2 5Gabriel LazarОценок пока нет
- Oral Surgery: Root Tip Migration Into The Infundibulum of The Maxillary Sinus After Complicated First Molar ExtractionДокумент4 страницыOral Surgery: Root Tip Migration Into The Infundibulum of The Maxillary Sinus After Complicated First Molar ExtractionGabriel LazarОценок пока нет
- BookRev 5 2 3Документ1 страницаBookRev 5 2 3Gabriel LazarОценок пока нет
- Teledentistry Your Partner in Improving The Oral Health Care of Your PatientsДокумент1 страницаTeledentistry Your Partner in Improving The Oral Health Care of Your PatientsGabriel LazarОценок пока нет
- Shortcuts in Esthetic DentistryДокумент1 страницаShortcuts in Esthetic DentistryGabriel Lazar100% (1)
- Computerized Dental Prosthetics: Intraoral Scans For Cad/Cam ApplicationДокумент8 страницComputerized Dental Prosthetics: Intraoral Scans For Cad/Cam ApplicationGabriel LazarОценок пока нет
- Article 5 4 1 PDFДокумент10 страницArticle 5 4 1 PDFGabriel LazarОценок пока нет
- Color in Dentistry A Clinical Guide To Predictable EstheticsДокумент1 страницаColor in Dentistry A Clinical Guide To Predictable EstheticsGabriel LazarОценок пока нет
- Contemporary Esthetic Dentistry, 1E (2012) (PDF) (UnitedVRG) PDFДокумент827 страницContemporary Esthetic Dentistry, 1E (2012) (PDF) (UnitedVRG) PDFAna Rahău100% (8)
- Proforma-I (A) Statement Showing Course-Wise Distribution of Students in Banaras Hindu University For The Session 2013-2014Документ340 страницProforma-I (A) Statement Showing Course-Wise Distribution of Students in Banaras Hindu University For The Session 2013-2014vineetОценок пока нет
- List BibliographyДокумент10 страницList BibliographyFabian BarretoОценок пока нет
- Margie Grether Resume 2019Документ1 страницаMargie Grether Resume 2019api-463132435Оценок пока нет
- Vertical Dimension and Freeway SpaceДокумент11 страницVertical Dimension and Freeway SpaceKanchit SuwanswadОценок пока нет
- Taub - Reconstruction of Marginal Mandibular Defects Utilizing Bone MarrДокумент1 страницаTaub - Reconstruction of Marginal Mandibular Defects Utilizing Bone MarrChristopher McMullinОценок пока нет
- Burkets Oral Medicine 13Th Edition Michael Glick Full ChapterДокумент51 страницаBurkets Oral Medicine 13Th Edition Michael Glick Full Chapterdavid.drew550100% (3)
- Dental Officer Information - e (1989)Документ10 страницDental Officer Information - e (1989)Marian GarciaОценок пока нет
- Dental Colleges in IndiaДокумент15 страницDental Colleges in IndiakannadiparambaОценок пока нет
- Be It Enacted by The Senate and House of Representatives of The Philippine Congress AssembledДокумент9 страницBe It Enacted by The Senate and House of Representatives of The Philippine Congress AssembledKarlvindeCardoОценок пока нет
- Good MorningДокумент26 страницGood MorningManoj KashyapОценок пока нет
- 5 6237874831283454643Документ425 страниц5 6237874831283454643Hady SpinОценок пока нет
- College Drive Dental Spring 2013 NewsletterДокумент4 страницыCollege Drive Dental Spring 2013 NewsletterDave HansenОценок пока нет
- Summer Dateline 2016Документ24 страницыSummer Dateline 2016indydentalsocietyОценок пока нет
- Germantown Express News 050413Документ24 страницыGermantown Express News 050413Hometown Publications - Express NewsОценок пока нет
- Universal AdhesivesДокумент5 страницUniversal AdhesivesSamuel Flores CalderonОценок пока нет
- Carranza's Clinical Periodontology (2nd Southeast Asian Edition)Документ978 страницCarranza's Clinical Periodontology (2nd Southeast Asian Edition)Janani Bendala84% (38)
- BDS Regulations HAND BOOK 2013-14 PDFДокумент135 страницBDS Regulations HAND BOOK 2013-14 PDFSayeeda MohammedОценок пока нет
- Corona OPD Consultant Directory 2020 1Документ5 страницCorona OPD Consultant Directory 2020 1rizviabbas2010Оценок пока нет
- A.T. Abimbola 178228Документ20 страницA.T. Abimbola 178228Oluwademilade AfolabiОценок пока нет
- Draft RegulationДокумент36 страницDraft RegulationPraveen TagoreОценок пока нет
- Sujeet Constitutional Law II AssignmentДокумент9 страницSujeet Constitutional Law II AssignmentSujeet kumarОценок пока нет
- Course Fees: 2022-23 Batch Total Fee Fee Caution Deposit TotalДокумент17 страницCourse Fees: 2022-23 Batch Total Fee Fee Caution Deposit TotalAnvith Ashoka KingsОценок пока нет
- TADs - NandaДокумент437 страницTADs - NandaPrabhu Thurai90% (21)
- R SunderДокумент3 страницыR SunderArvind prabu KОценок пока нет
- Escorts Agri Faridabad - Process of Production of Rear Axle - Mechanical Engg. (ME) Summer InnternshipДокумент34 страницыEscorts Agri Faridabad - Process of Production of Rear Axle - Mechanical Engg. (ME) Summer InnternshipVinnie SinghОценок пока нет
- Polyetheretherketone in Implant Prosthodontics: A Scoping ReviewДокумент9 страницPolyetheretherketone in Implant Prosthodontics: A Scoping ReviewNelson BarakatОценок пока нет
- Abeginningguidefor Dentalphotography: A Simplified Introduction For Esthetic DentistryДокумент28 страницAbeginningguidefor Dentalphotography: A Simplified Introduction For Esthetic DentistryChrissie GutierrezОценок пока нет
- MU Prospectus 2016 RevisedДокумент184 страницыMU Prospectus 2016 RevisedRico BuffetОценок пока нет
- Revaluation RulesДокумент3 страницыRevaluation Rulesਗਗਨ ਦੀਪ ਸਿੰਘОценок пока нет