Вам также может понравиться
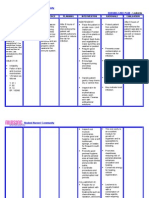
- NURSING CARE PLAN 1 - Written ReportДокумент4 страницыNURSING CARE PLAN 1 - Written ReportAkira PinedaОценок пока нет
- Hyper-Pigmentation Of The Skin A Simple Guide To The Condition, Treatment, And Related ConditionsОт EverandHyper-Pigmentation Of The Skin A Simple Guide To The Condition, Treatment, And Related ConditionsРейтинг: 5 из 5 звезд5/5 (3)
- NCP On BURNS - LECOBU-ANДокумент3 страницыNCP On BURNS - LECOBU-ANMae Arra Lecobu-anОценок пока нет
- NCP - Impaired Skin IntegrityДокумент3 страницыNCP - Impaired Skin IntegrityFlauros Ryu Jabien90% (29)
- NCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)Документ2 страницыNCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)yanny0350% (2)
- Impaired Skin DMДокумент3 страницыImpaired Skin DMimnotdatsunny100% (1)
- 12 NCPДокумент3 страницы12 NCPKate ChavezОценок пока нет
- College of Nursing and Allied Medical Sciences: WesleyanДокумент3 страницыCollege of Nursing and Allied Medical Sciences: WesleyanCharie OcampoОценок пока нет
- NCP Impaired SkinДокумент2 страницыNCP Impaired Skinarjay2306_obcq100% (1)
- Nursing Care Plan-AguilarДокумент3 страницыNursing Care Plan-AguilarphearlieОценок пока нет
- Risk For Infection Related To High Glucose LevelsДокумент2 страницыRisk For Infection Related To High Glucose LevelsDanica Kate GalleonОценок пока нет
- NCP 1 CSДокумент2 страницыNCP 1 CSjuliechan_17mjОценок пока нет
- NCP Template W InferenceДокумент5 страницNCP Template W InferenceVannesa TarifaОценок пока нет
- NCP Rectal AdenocarcinomaДокумент3 страницыNCP Rectal AdenocarcinomaReysiela Mae ValinoОценок пока нет
- SJS NCPДокумент4 страницыSJS NCPAira Alaro50% (2)
- Assessment Diagnosis Planning Implementation Rationale EvaluationДокумент2 страницыAssessment Diagnosis Planning Implementation Rationale EvaluationGlare RhayneОценок пока нет
- Nursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationДокумент23 страницыNursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationTweenie DalumpinesОценок пока нет
- Assessment Nursing Diagnosis Planning Intervention Evaluation ObjectivesДокумент4 страницыAssessment Nursing Diagnosis Planning Intervention Evaluation Objectivesashamy acolОценок пока нет
- Nursing Care Plan For Tissue InjuryДокумент2 страницыNursing Care Plan For Tissue InjuryJobelle AcenaОценок пока нет
- Diabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleДокумент11 страницDiabetes Mellitus Client "Nursing Care Plan": Assesment Nursing Diagnosis Planning Nursing Interventions RationaleKatherine_Chyr_9112Оценок пока нет
- Nursing Care Plan: Subjective Data: Short Term Goal: Independent Nursing ActionДокумент2 страницыNursing Care Plan: Subjective Data: Short Term Goal: Independent Nursing ActionIzhiel AbadОценок пока нет
- Nursing Care Plan LeukemiaДокумент2 страницыNursing Care Plan Leukemiaderic87% (30)
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG Independent STДокумент4 страницыAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG Independent STFrando kennethОценок пока нет
- NCP2Документ2 страницыNCP2Jrose CuerpoОценок пока нет
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationДокумент2 страницыAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationDuane LilocОценок пока нет
- Nursing Care Plan DM Type 2Документ3 страницыNursing Care Plan DM Type 2Jay V. FranciscoОценок пока нет
- NCPPPPPPPPZДокумент12 страницNCPPPPPPPPZKANT JAMES D. MAHANОценок пока нет
- Impaired Skin Integrity For NCP Oct. 212020Документ2 страницыImpaired Skin Integrity For NCP Oct. 212020Benjie DimayacyacОценок пока нет
- Assessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermДокумент2 страницыAssessme NT Diagnosis Planning Intervention Rational E Evaluation Subjectiv E: Short Term: Independent: Short TermPeter Emmil GonzalesОценок пока нет
- Nursing Care Plan FormДокумент3 страницыNursing Care Plan FormHanniel MontecalboОценок пока нет
- NCP Bed SoresДокумент3 страницыNCP Bed SoresShe CalliОценок пока нет
- Group 4 NCPДокумент9 страницGroup 4 NCPJames De VeraОценок пока нет
- Nursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term GoalsДокумент3 страницыNursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term GoalsdanicaОценок пока нет
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationДокумент5 страницNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaОценок пока нет
- Nursing Care PlanДокумент10 страницNursing Care PlanIsabelle Madrid100% (1)
- Cellulitis NCPДокумент4 страницыCellulitis NCPcataleya mesaОценок пока нет
- Cebu Institute of Technology - University College of NursingДокумент2 страницыCebu Institute of Technology - University College of NursingSergi Lee OrateОценок пока нет
- Davao Doctors College General Malvar Street, Davao City Nursing ProgramДокумент5 страницDavao Doctors College General Malvar Street, Davao City Nursing ProgramJhoneric Vencer EscultorОценок пока нет
- NCP ImpairedДокумент3 страницыNCP ImpairedLyka NgayanОценок пока нет
- NCP 2 Impaired Skin Integrity EDITEDДокумент2 страницыNCP 2 Impaired Skin Integrity EDITEDVincent HermanoОценок пока нет
- NCP 2 - CellulitisДокумент4 страницыNCP 2 - CellulitisROSHANNEDANICA VERGARAОценок пока нет
- IX. Nursing Care PlanДокумент7 страницIX. Nursing Care PlanMunisa M. UsmanОценок пока нет
- NCP Impaired Skin IntegrityДокумент3 страницыNCP Impaired Skin IntegrityMiar QuestОценок пока нет
- NCP Impaired Tissue IntegrityДокумент4 страницыNCP Impaired Tissue IntegrityKingJayson Pacman06Оценок пока нет
- NCP Impaired Skin IntergrityДокумент2 страницыNCP Impaired Skin IntergrityDianna RoseОценок пока нет
- NURSING CARE PLAN 2 - Written ReportДокумент3 страницыNURSING CARE PLAN 2 - Written ReportAkira PinedaОценок пока нет
- 2nd-Sem-Micro-Lab 2Документ3 страницы2nd-Sem-Micro-Lab 2Kristine Angie RamosОценок пока нет
- Assessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Документ4 страницыAssessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Arian May MarcosОценок пока нет
- Nursing CheepeeeДокумент2 страницыNursing CheepeeesynaPtiCjeRkОценок пока нет
- Fdar NCPДокумент16 страницFdar NCPshiОценок пока нет
- Pascua NCPДокумент2 страницыPascua NCPLawrene Landingin IralОценок пока нет
- Nursing Care Plan Cues Nursing Diagnosis Analysis Goal Intervention Rationale Evaluatio NДокумент3 страницыNursing Care Plan Cues Nursing Diagnosis Analysis Goal Intervention Rationale Evaluatio NAishleen OrmandoОценок пока нет
- Impaired Skin IntegrityДокумент2 страницыImpaired Skin IntegrityEli AyaseОценок пока нет
- COAD Prelim RevДокумент4 страницыCOAD Prelim RevNhica GrandeОценок пока нет
- Nursing Care Plan For Wound HealingДокумент2 страницыNursing Care Plan For Wound HealingJobelle Acena50% (2)
- For Printing Jan23Документ3 страницыFor Printing Jan23Jhoan OllanoОценок пока нет
- NCP Cholelithiasis Impaired Skin IntegrityДокумент3 страницыNCP Cholelithiasis Impaired Skin IntegrityReysiela Mae ValinoОценок пока нет
- CA Risk For Infection NCPДокумент2 страницыCA Risk For Infection NCPJheanAlphonsineT.MeansОценок пока нет
- NCP 1 - Chicken PoxДокумент2 страницыNCP 1 - Chicken Poxphearlie100% (2)
- Letter of ProfessionalismДокумент1 страницаLetter of ProfessionalismDerick RanaОценок пока нет
- Diabetes Group ReportДокумент34 страницыDiabetes Group ReportDerick RanaОценок пока нет
- Smith L (2017) Nursing Times 113: 12, 20-23Документ59 страницSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaОценок пока нет
- Ic-01-047 Infection Control in Operating RoomДокумент13 страницIc-01-047 Infection Control in Operating RoomDerick RanaОценок пока нет
- Diabetes Nursing EducationДокумент4 страницыDiabetes Nursing EducationDerick RanaОценок пока нет
- Policies and Procedures Manual Infection Control in General Nursing UnitДокумент9 страницPolicies and Procedures Manual Infection Control in General Nursing UnitDerick RanaОценок пока нет
- Ic-01-049 Infection Control in Clinical EngineeringДокумент4 страницыIc-01-049 Infection Control in Clinical EngineeringDerick RanaОценок пока нет
- Ic-01-039 Infection Control in Adult Intensive Care UnitДокумент7 страницIc-01-039 Infection Control in Adult Intensive Care UnitDerick RanaОценок пока нет
- Ic-01-040 Infection Control in Dental ClinicДокумент11 страницIc-01-040 Infection Control in Dental ClinicDerick RanaОценок пока нет
- Ic-01-048 Infection Control in Pediatric Intensive Care UnitДокумент6 страницIc-01-048 Infection Control in Pediatric Intensive Care UnitDerick RanaОценок пока нет
- Ic-01-041 Infection Control in DialysisДокумент15 страницIc-01-041 Infection Control in DialysisDerick RanaОценок пока нет
- Ic-01-042 Infection Control in Emergency RoomДокумент13 страницIc-01-042 Infection Control in Emergency RoomDerick RanaОценок пока нет
- Ohhc Obtaining Stool Specimens For Laboratory AnalysisДокумент8 страницOhhc Obtaining Stool Specimens For Laboratory AnalysisDerick RanaОценок пока нет
- Smith L (2017) Nursing Times 113: 12, 20-23Документ59 страницSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaОценок пока нет
- Critical Care Notes BookДокумент142 страницыCritical Care Notes BookDerick RanaОценок пока нет
- Recruitment Checklist: Security Forces Hospital ProgramДокумент4 страницыRecruitment Checklist: Security Forces Hospital ProgramDerick RanaОценок пока нет
- Emergency NursingДокумент5 страницEmergency NursingDerick RanaОценок пока нет
- Policies and Procedures Manual Tube Feeding (Nasogastic)Документ5 страницPolicies and Procedures Manual Tube Feeding (Nasogastic)Derick RanaОценок пока нет
- DEMENTIA Citical ExamДокумент4 страницыDEMENTIA Citical ExamDerick RanaОценок пока нет
- Policies and Procedures Manual Tube FeedingДокумент4 страницыPolicies and Procedures Manual Tube FeedingDerick RanaОценок пока нет
- Ohhc Laboratory ProceduresДокумент3 страницыOhhc Laboratory ProceduresDerick RanaОценок пока нет
- Ohhc Clean CatchДокумент5 страницOhhc Clean CatchDerick RanaОценок пока нет
- DOH Standards (Indicators)Документ2 страницыDOH Standards (Indicators)Derick RanaОценок пока нет
- Job Description: 1.1 Professional, Ethical and LegalДокумент11 страницJob Description: 1.1 Professional, Ethical and LegalDerick RanaОценок пока нет
- NX Service Admin Practicum Packet-1Документ12 страницNX Service Admin Practicum Packet-1Derick RanaОценок пока нет
- New Microsoft Office Word DocumentДокумент102 страницыNew Microsoft Office Word DocumentResearch Center for Training and DevelopmentОценок пока нет
- NCP FormДокумент3 страницыNCP FormJasmine diokОценок пока нет
- Summary of Product Characteristics: PosologyДокумент9 страницSummary of Product Characteristics: Posologyddandan_2Оценок пока нет
- Drowsiness Detection System Using OpenCV and PythonДокумент10 страницDrowsiness Detection System Using OpenCV and Pythonsharath srivatsanОценок пока нет
- Driver Drowsiness Abstract ReviewДокумент13 страницDriver Drowsiness Abstract ReviewAishwarya MyadamОценок пока нет
- Internship Report On Stress Management AДокумент52 страницыInternship Report On Stress Management ARiyad HossenОценок пока нет
- Nursing Care PlanДокумент28 страницNursing Care PlanChristine Karen Ang Suarez67% (3)
- Locomotor Muscles COPDДокумент15 страницLocomotor Muscles COPDAllison Medrano PinedaОценок пока нет
- Cross-Cultural Conflict AdjustmentДокумент27 страницCross-Cultural Conflict Adjustmenttapdew 25Оценок пока нет
- NCM 103 ReviewerДокумент10 страницNCM 103 ReviewerFiona GungonОценок пока нет
- Trial Summary Evaluation Bahan Bacaan Soalan Sem 1 2020-2021Документ6 страницTrial Summary Evaluation Bahan Bacaan Soalan Sem 1 2020-2021Caren JasonОценок пока нет
- TopstepTrader Path Funded Trader EbookДокумент26 страницTopstepTrader Path Funded Trader EbookfnopulseОценок пока нет
- P S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care PlanДокумент1 страницаP S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care Planunkown userОценок пока нет
- MS SymptomsДокумент2 страницыMS SymptomsVennice Dela PenaОценок пока нет
- ComplicenceДокумент8 страницComplicencekivОценок пока нет
- Final Research PaperДокумент89 страницFinal Research PaperStar100% (1)
- Jonathan Edwards TrainingДокумент8 страницJonathan Edwards TrainingMark100% (1)
- De 3Документ15 страницDe 3stillaphenomenonОценок пока нет
- 13 Areas of Assessment (Tomas Claudio Memorial College)Документ14 страниц13 Areas of Assessment (Tomas Claudio Memorial College)jorden36067% (3)
- CHIRP Perception Decision Making and Fatigue at Sea 2018 01Документ16 страницCHIRP Perception Decision Making and Fatigue at Sea 2018 01Mithran DirОценок пока нет
- n703 Chronic Soap NoteДокумент3 страницыn703 Chronic Soap NoteJeffrey ViernesОценок пока нет
- Current Status of Sports FacilitiesДокумент5 страницCurrent Status of Sports FacilitiesMike Gonzales JulianОценок пока нет
- Seagull CD0399 Fatigue Management - Good LeadershipДокумент3 страницыSeagull CD0399 Fatigue Management - Good LeadershipАнди Анди100% (1)
- Social Media Influence in AdolescenceДокумент20 страницSocial Media Influence in Adolescencealphonsa kuriakoseОценок пока нет
- AQA A-Level Psychology PYA5: Clinical CharacteristicsДокумент3 страницыAQA A-Level Psychology PYA5: Clinical CharacteristicsStephan Amaranath100% (1)
- FatigueДокумент26 страницFatigueAbdulbari AL-GhamdiОценок пока нет
- Related To Vomiting As Evidence by Muscle Weakness and FatigueДокумент3 страницыRelated To Vomiting As Evidence by Muscle Weakness and FatiguejuiceОценок пока нет
- DD ADHS - DepressionДокумент4 страницыDD ADHS - DepressionMaria F Martinez LeanesОценок пока нет
- Bài Reading B Sung HP SauДокумент23 страницыBài Reading B Sung HP SauTrangОценок пока нет
- Diagnostic ActivityДокумент3 страницыDiagnostic ActivityTantan YbañezОценок пока нет