Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- BeneFusion VP1&VP3 - Service Manual - V1.0 - ENДокумент61 страницаBeneFusion VP1&VP3 - Service Manual - V1.0 - ENkellyng jinete71% (7)
- Haad QuestionsДокумент8 страницHaad QuestionsBio EstonactocОценок пока нет
- O 6Документ4 страницыO 6nitaОценок пока нет
- KCL Medication Safety AlertДокумент3 страницыKCL Medication Safety AlertokiОценок пока нет
- IV Fluid Management: Islam Awni Abu SamraДокумент41 страницаIV Fluid Management: Islam Awni Abu SamraIslam AwniОценок пока нет
- CVC Train Module1Документ28 страницCVC Train Module1Daniel SusantoОценок пока нет
- Study MaterialДокумент145 страницStudy Materialmalikmohsin007.mmОценок пока нет
- Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is SuspectedДокумент19 страницClinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is SuspectedgustixОценок пока нет
- ASHP PCA and Epidural StandardsДокумент20 страницASHP PCA and Epidural StandardsJessica TorreglosaОценок пока нет
- Bahasa Inggris Kelompok SyahdanДокумент11 страницBahasa Inggris Kelompok SyahdanAji cupleeОценок пока нет
- IPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyДокумент27 страницIPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyEvangelin MelvinОценок пока нет
- IV Catheter Insertion PDFДокумент17 страницIV Catheter Insertion PDFHannaОценок пока нет
- CVPДокумент3 страницыCVPAudreySalvadorОценок пока нет
- Maria Ivy Rochelle S. Tan, BSN-RN: Specialization: Pacu/Or /erДокумент9 страницMaria Ivy Rochelle S. Tan, BSN-RN: Specialization: Pacu/Or /erNoel FuentesОценок пока нет
- (P.T) Preparing The IV Bag and TubingДокумент2 страницы(P.T) Preparing The IV Bag and TubingThao NguyenОценок пока нет
- Medical Surgical ChecklistДокумент9 страницMedical Surgical ChecklistAnonymous aNQoi7h9Оценок пока нет
- Flashcards for Admin ConsiderationsДокумент1 страницаFlashcards for Admin ConsiderationsAntonette Joy SolinapОценок пока нет
- Final Report-Vein Finder DeviceДокумент52 страницыFinal Report-Vein Finder DeviceIbsa GetachoОценок пока нет
- Yovita - The Role of Clinical Pharmacist On Safe Administration AntibioticДокумент48 страницYovita - The Role of Clinical Pharmacist On Safe Administration AntibioticRois HasyimОценок пока нет
- Manual RleДокумент25 страницManual RleMark Jason P DiazОценок пока нет
- Cardinal Alaris-GW - Service ManualДокумент81 страницаCardinal Alaris-GW - Service ManualassistenciaОценок пока нет
- Antibiotics in NeurosurgeryДокумент12 страницAntibiotics in Neurosurgerylouglee9174100% (1)
- Iv Procedure ChecklistДокумент2 страницыIv Procedure ChecklistCYRIL YANNA MENDONESОценок пока нет
- Laboratory Animal Handling Technique: - Mouse - Rat - RabbitДокумент36 страницLaboratory Animal Handling Technique: - Mouse - Rat - RabbitAnonymous RHwDUfBavUОценок пока нет
- Oxaliplatin Monograph 1dec2016Документ9 страницOxaliplatin Monograph 1dec2016Nadial UzmahОценок пока нет
- Drug Calculations AssignmentДокумент8 страницDrug Calculations AssignmentBern NerquitОценок пока нет
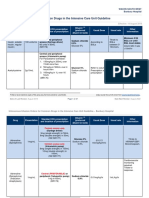
- Intravenous Infusion Orders For Common Drugs in The Intensive Care Unit Guideline - Bunbury HospitalДокумент37 страницIntravenous Infusion Orders For Common Drugs in The Intensive Care Unit Guideline - Bunbury HospitalCristian Sandoval RojasОценок пока нет
- Gram Negative SepsisДокумент12 страницGram Negative SepsisDima GheorgheОценок пока нет
- IV Fluid Replacement TherapyДокумент12 страницIV Fluid Replacement TherapyKamran Sheraz100% (1)
- Recording of Fluid Balance Intake-Output PolicyДокумент7 страницRecording of Fluid Balance Intake-Output PolicyRao Rizwan ShakoorОценок пока нет